
The Association of Minimally Invasive Gynecologic Surgeons
…dedicated to safe, state-of-the-art surgery and health life-styles for women of all ages
Can Breast Cancer Be Found Early?
Screening refers to tests and exams used to detect a disease, such as cancer, in people who do not have any
symptoms. The goal of screening exams, such as mammograms, for early breast cancer detection is to find
cancers before they start to cause symptoms. Breast cancers that are detected because they can be felt tend to be
larger and are more likely to have spread beyond the breast. In contrast, breast cancers found during screening
examinations are more likely to be small and still confined to the breast.
The size of a breast cancer and how far it has spread are the most important factors in predicting the prognosis (the
outlook for chances of survival) of a woman with this disease. Finding a breast cancer as early as possible
improves the likelihood that treatment will be successful. Most doctors feel that early detection tests for breast
cancer save many thousands of lives each year, and that many more lives could be saved if even more women and
their health care providers took advantage of these tests. Following the American Cancer Society's guidelines for
the early detection of breast cancer improves the chances that breast cancer can be diagnosed at an early stage
and treated successfully.
American Cancer Society Recommendations for Early Breast Cancer Detection
Women age 40 and older should have a screening mammogram every year and should continue to do so for as
long as they are in good health.
Current evidence supporting mammograms is even stronger than in the past. In particular, recent evidence
has confirmed that mammograms offer substantial benefit for women in their 40s. Women can feel
confident about the benefits associated with regular mammograms for finding cancer early. However,
mammograms also have limitations. A mammogram will miss some cancers, and it sometimes leads to
follow up of findings that are not cancer, including biopsies.
Women should be told about the benefits, limitations, and potential harms linked with regular screening.
Mammograms can miss some cancers. However, mammograms, despite their limitations, remain a very
effective and valuable tool for decreasing suffering and death from breast cancer.
Mammograms for older women should be based on the individual, her health, and other serious illnesses,
such as congestive heart failure, end-stage renal disease, chronic obstructive pulmonary disease, and
moderate-to-severe dementia. Age alone should not be the reason to stop having regular mammograms.
As long as a woman is in good health and would be a candidate for treatment, she should continue to be
screened with a mammogram.
Women in their 20s and 30s should have a clinical breast exam (CBE) as part of a periodic (regular) health exam
by a health professional preferably every 3 years. After age 40, women should have a breast exam by a health
p
rofessional every year.
CBE is a complement to mammograms and an opportunity for women and their doctor or nurse to discuss
changes in their breasts, early detection testing, and factors in the woman’s history that might make her
more likely to have breast cancer.
There may be some benefit in having the CBE shortly before the mammogram. The exam should include
instruction for the purpose of getting more familiar with your own breast. Women should also be given
information about the benefits and limitations of CBE and breast self exam (BSE). Breast cancer risk is
very low for women in their 20s and gradually increases with age. Women should be told to promptly report
any new breast symptoms to a health professional.
BSE is an option for women starting in their 20s. Women should be told about the benefits and limitations of BSE.
Women should report any breast changes to their health professional right away.
Research has shown that BSE plays a small role in finding breast cancer compared with finding a breast
lump by chance or simply being aware of what is normal for each woman. Some women feel very
comfortable doing BSE regularly (usually monthly) which involves a systematic step-by-step approach to
examining the look and feel of one’s breasts. Other women are more comfortable simply looking and
feeling their breasts in a less systematic approach, such as while showering or getting dressed or doing an
occasional thorough exam. Sometimes, women are so concerned about "doing it right" that they become
stressed over the technique. Doing BSE regularly is one way for women to know how their breasts normally
look and feel and to notice any changes. The goal, with or without BSE, is to report any breast changes to
a doctor or nurse right away.
Women who choose to do BSE should have their BSE technique reviewed during their physical exam by a
health professional. It is okay for women to choose not to do BSE or not to do it on a regular schedule.
However, by doing the exam regularly, you get to know how your breasts normally look and feel and you
can more readily detect any signs or symptoms If a change occurs, such as development of a lump or
swelling, skin irritation or dimpling, nipple pain or retraction (turning inward), redness or scaliness of the
nipple or breast skin, or a discharge other than breast milk. Should you notice any changes you should see
your health care provider as soon as possible for evaluation. Remember that most of the time, however,
these breast changes are not cancer.
Women at increased risk should talk with their doctors about the benefits and limitations of starting mammograms
when they are younger, having additional tests (such as breast ultrasound or MRI), or having more frequent exams.
All women are at risk for breast cancer and the risk increases as women get older, especially after age 40.
Some women have other factors that increase their likelihood of breast cancer more than most women.
The evidence available for women at increased risk can only offer general guidance to help women and
their doctors make more informed decisions about finding breast cancer early. Women should discuss with
their doctor what approaches are best for them.
Most recent studies have found that magnetic resonance imaging (MRI) is the most sensitive test for
detecting breast cancer in women at high risk of the disease. Although the evidence currently available is
not sufficient to make a recommendation for or against the use of breast ultrasound or MRI for screening,
women at increased risk and their doctors can discuss what is known (the benefits and limitations of these
tests) and make the best decision for each individual. If one of these tests is used, it should be used in
addition to, not instead of, a screening mammogram. It is also recommended that women who choose one
of these testing methods do so as part of a research study if possible, so that more data can be collected
on the usefulness of these tests.
The American Cancer Society believes the use of mammograms, clinical breast exam, and finding and reporting
breast changes early, according to the recommendations outlined above, offers women the best opportunity for
reducing the breast cancer death rate through early detection. This combined approach is clearly better than any
one examination. Without question, breast physical exam without a mammogram would miss the opportunity to
detect many breast cancers that are too small for a woman or her doctor to feel, but can be seen on mammograms.
While mammograms are the most sensitive screening method, a small percentage of breast cancers do not show
up on mammograms, but can be felt by a woman or her doctors. For women at high risk of breast cancer, such as
those with BRCA mutations or a strong family history, many breast cancer specialists are recommending both MRI
and mammogram exams of the breast.
Mammograms
A mammogram is an x-ray of the breast. A diagnostic mammogram is used to diagnose breast disease in women
who have breast symptoms. Screening mammograms are used to look for breast disease in women who are
asymptomatic; that is, they appear to have no breast problems. Screening mammograms usually involve 2 views
(x-ray pictures) of each breast. For some patients, such as women with breast implants, additional pictures may be
needed to include as much breast tissue as possible. Women who are breast-feeding can still get mammograms,
although these are probably not quite as accurate.
Although breast x-rays have been performed for more than 70 years, the modern mammogram has only existed
since 1969. That was the first year x-ray units specifically for breast imaging were available. Modern mammogram
equipment designed for breast x-rays uses very low levels of radiation, usually a dose of about 0.1 to 0.2 rads per
picture.
Strict guidelines are in place to ensure that mammogram equipment is safe and uses the lowest dose of radiation
possible. Many people are concerned about the exposure to x-rays, but the level of radiation used in modern
mammograms does not significantly increase the risk for breast cancer.
To put dose into perspective, if a woman with breast cancer is treated with radiation, she will receive around 5,000
rads (a rad is a measure of radiation dose). If she had yearly mammograms beginning at age 40 and continuing
until she was 90, she will have received 20 to 40 rads. As another example, flying from New York to California on a
commercial jet exposes a woman to roughly the same amount of radiation as one mammogram.
For a mammogram, the breast is pressed between 2 plates to flatten and spread the tissue. Although this may be
uncomfortable for a moment, it is necessary to produce a good, "readable" mammogram. The compression only
lasts a few seconds. The entire procedure for a screening mammogram takes about 20 minutes. This procedure
produces a black and white image of the breast tissue on a large sheet of film that is read, or interpreted, by a
radiologist (a doctor specially trained to interpret images from x-rays, ultrasound, MRI, and related tests).
The doctor reading the films will look for several types of changes:
Calcifications, or microcalcifications, are tiny mineral deposits within the breast tissue that appear as
small white spots on the film. They may occur singly or in clusters. They are a sign of changes within the
breast and can be either carefully watched by additional, periodic mammograms or examined by biopsy
(removal of a small amount of breast tissue). They may be caused by benign breast conditions or, less
often, by breast cancer.
A mass, which may occur with or without calcifications, is another important change that can be seen on a
mammogram. Masses can be many things, including cysts and fibroadenomas, but they may be cancer
and usually should be biopsied.
A cyst is a collection of fluid in a small sac in the breast. It can feel like a lump, usually soft, in the breast.
Either a breast ultrasound or removal of the fluid with a needle (aspiration) is used to confirm that a mass,
or lump, is a cyst and not another type of mass. It is very rare for a cyst to be cancerous. If a cyst has
ultrasound features that are suggestive of cancer, fluid removed from the cyst will be examined to look for
malignant cells or an ultrasound-guided biopsy of the suspicious region of the cyst will be performed.
A mammogram cannot prove that an abnormal area is cancer. To confirm whether cancer is present, a small
amount of tissue must be removed and examined under a microscope. This procedure is called a biopsy.
You should also be aware that mammograms are imperfect at finding breast cancer. If you have a breast lump, you
should have it checked by your doctor and consider having it biopsied even if your mammogram is normal.
For some women, such as those with breast implants (for augmentation or as reconstruction after mastectomy),
additional pictures may be needed to include as much breast tissue as possible. Breast implants make it harder to
see breast tissue on standard mammograms, but additional x-ray pictures with implant displacement and
compression views can be used to more completely examine the breast tissue.
Finally, mammograms are less effective in younger women, usually because their breasts are dense and this can
hide a tumor. This is also true for pregnant women and women who are breast feeding, although studies have
shown that the breasts may or may not be any denser than before their pregnancy. Since most breast cancers
occur in older women, this is usually not a major problem. It is, however, a problem for young women who have a
genetic risk factor for breast cancer because they often develop breast cancer at a younger age. For this reason,
some doctors are now suggesting MRI in addition to mammograms for screening in this population of women.
For more information see the American Cancer Society document, "Mammograms and Other Breast Imaging
Procedures."
When You Get a Mammogram
Medicare, Medicaid, and most private health insurance plans cover mammogram costs or a percentage of them.
Low-cost mammograms are available in most communities. Call us at 1-800-ACS-2345 for information about
facilities in your area.
The procedure requires that you undress above the waist. A wrap for you to wear will be provided by the facility.
A technologist will be present to position your breasts for the mammogram. Most technologists are women. You
and the technologist are the only ones present during the mammogram. Women who have no breast lumps or
symptoms will have a screening mammogram. This includes 2 pictures of each breast, a top to bottom and a side-
to-side view. To get a high-quality mammogram picture with excellent image quality, it is necessary to flatten the
breast slightly. A technician places the breast on the mammogram machine’s lower plate, which is made of metal
and has a drawer to hold the x-ray film. The upper plate, made of clear plastic, is lowered to compress the breast
for a few seconds while the technician takes a picture. Although compression may be uncomfortable, most women
do not say it is painful.
The whole procedure takes about 20 minutes. The actual breast compression only lasts a few seconds.
You may feel some discomfort when your breasts are compressed, but you should not feel pain. Try not to
schedule a mammogram when your breasts are likely to be tender, as they may be just before or during your
period.
All mammography facilities are now required to send your results to you within 30 days. You will be contacted
within 5 working days if there is a problem with the mammogram.
Only 1 or 2 mammograms of every 1,000 lead to a diagnosis of cancer. However, about 10% of women will require
additional mammograms. Don't be alarmed if this happens to you. Only 8% to 10% of those women will need a
biopsy, and 80% of those biopsies will not be cancer.
If you are a woman aged 40 or over, you should get a mammogram every year. You can schedule the next one
while you're at the facility and/or request a reminder.
Tips for Mammograms
The following are useful suggestions for making sure that you will receive a quality mammogram:
Ask to see the FDA certificate that is issued to all facilities that meet high professional standards of safety
and quality.
Use a facility that either specializes in mammograms or performs at least 3 to 5 mammograms a day.
If you are satisfied that the facility is of high quality, continue to go there on a regular basis so that your
mammograms can be compared from year to year.
If you change facilities, it is important to take your previous mammograms with you to the new facility so
that they can be compared to the new ones.
If you have sensitive breasts, try having your mammogram at a time of the month when your breasts will be
least tender. Try to avoid the week right before your period. This will help lessen the discomfort.
Don't wear deodorant, powder, or cream under your arms -- it may interfere with the quality of the
mammogram.
Bring a list of the places, dates of mammograms, biopsies, or other breast treatments you have had before.
If you do not hear from your doctor within 10 days, do not assume that your mammogram was normal --
confirm this by calling your doctor or the facility.
Financial assistance for breast cancer testing for low-income women: Breast cancer testing is now more
available to medically underserved women through the National Breast and Cervical Cancer Early Detection
Program (NBCCEDP). This program provides breast and cervical cancer early detection testing to women without
health insurance for free or at very low cost.
The NBCCEDP attempts to reach as many women in medically underserved communities as possible, including
older women, women without health insurance, and women who are members of racial and ethnic minorities.
Although the program is administered within each state, the Centers for Disease Control and Prevention (CDC)
provide matching funds and support to each state program.
Offered mainly through nonprofit organizations and local health clinics, this program makes testing available for
breast and cervical cancer in medically underserved women. Each state's Department of Health has information on
how to contact the nearest program.
In 2000, the Breast and Cervical Cancer Treatment Act was signed into law. This act adds to the NBCCEDP by
providing funds to pay for treatment associated with breast and cervical cancer in medically underserved
populations. This new option helps women focus their energies on fighting their disease, instead of worrying about
how to pay for treatment. As with the Early Detection Program, individual states must adopt the program to receive
the matching federal funds.
The program is only designed to provide screening. But if a cancer is discovered, it will cover further diagnostic
testing and a surgical consultation.
To learn more about this program, please contact the CDC at 1-888-842-6355 or on the Internet at
www.cdc.gov/cancer.
Clinical Breast Exam
A clinical breast exam (CBE) is an exam of your breasts by a health care professional, such as a doctor, nurse
practitioner, nurse, or doctor's assistant. For this exam, you undress from the waist up. The health care professional
will first look at your breasts for changes in size or shape. Then, using the pads of the fingers, the examiner will
gently feel (palpate) your breasts.
Special attention will be given to the shape and texture of the breasts, location of any lumps, and whether such
lumps are attached to the skin or to deeper tissues. The area under both arms will also be examined.
During the CBE is a good time for the health care professional to teach breast self-examination to the woman who
does not already know how to examine her breasts. Ask your doctor or nurse to teach you and watch your
technique.
Breast Awareness and Self Exam
Beginning in their 20s, women should be told about the benefits and limitations of breast self exam (BSE). Women
should be aware of how their breasts normally look and feel and report any new breast change to a health
professional as soon as they are found. Finding a breast change does not mean there is a cancer.
Women can notice changes by being aware of how their breasts normally look and feel and by feeling their breasts
for changes (breast awareness) or by choosing to use a step-by-step approach (see below) and using a specific
schedule to examine her breasts.
Women with breast implants can do BSE. It may be helpful to have the surgeon help identify the edges of the
implant so that you know what you are feeling. There is some thought that the implants push out the breast tissue
and actually make it easier to examine.
If you choose to do BSE, the following information provides a step-by-step approach for the exam. The best time for
a woman to examine her breasts is when the breasts are not tender or swollen. Women who are pregnant, breast
feeding, or have breast implants can also choose to examine their breasts regularly. Women who examine their
breasts should have their technique reviewed during their periodic health exams by their health care professional. It
is acceptable for women to choose not to do BSE or to do BSE occasionally.
For women who choose not to do BSE, they should still be aware of their breasts and report any changes without
delay to their doctor.
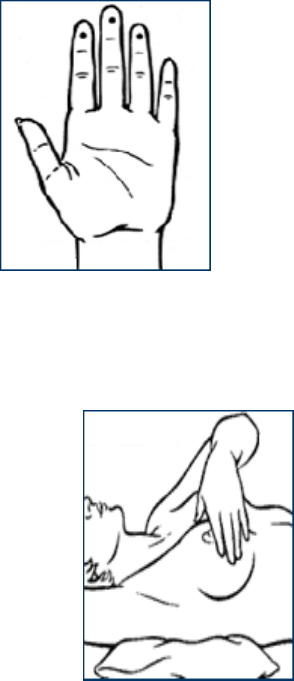
How to Examine Your Breasts
Lie down and place your right arm behind your head. The exam is done while lying
down, not standing up. This is because when lying down the breast tissue spreads
evenly over the chest wall and it is as thin as possible making it much easier to feel
all the breast tissue.
Use the finger pads of the 3 middle fingers on your left hand to feel for lumps in the
right breast. Use overlapping dime-sized circular motions of the finger pads to feel
the breast tissue.
Use 3 different levels of pressure to feel all the breast tissue. Light pressure is
needed to feel the tissue closest to the skin; medium pressure to feel a little deeper; and firm pressure to
feel the tissue closest to the chest and ribs. A firm ridge in the lower curve of each breast is normal. If
you're not sure how hard to press, talk with your doctor or nurse. Use each pressure to feel the breast
tissue before moving on to the next spot.
Move around the breast in an up and down pattern starting at an imaginary line drawn straight down your
side from the underarm and moving across the breast to the middle of the chest bone (sternum or
breastbone). Be sure to check the entire breast area going down until you feel only ribs and up to the neck
or collar bone (clavicle).
There is some evidence to suggest that the up and down pattern (sometimes called the vertical pattern) is
the most effective pattern for covering the entire breast, without missing any breast tissue.
Repeat the exam on your left breast, using the finger pads of the right hand.
While standing in front of a mirror with your hands pressing firmly down on your hips, look at your breasts
for any changes of size, shape, contour, or dimpling, or redness or scaliness of the nipple or breast skin.
(The pressing down on the hips position contracts the chest wall muscles and enhances any breast
changes.)
Examine each underarm while sitting up or standing and with your arm only slightly raised so you can
easily feel in this area. Raising your arm straight up tightens the tissue in this area and makes it difficult to
examine.
This procedure for doing breast self exam is different than in previous procedure recommendations. These changes
represent an extensive review of the medical literature and input from an expert advisory group. There is evidence
that the woman's position (lying down), area felt, pattern of coverage of the breast, and use of different amounts of
pressure increase the sensitivity of BSE as measured with silicone models. Lying down also increased the
sensitivity of CBE using patient models with known small non-cancerous lumps in their breasts.