R. Wayne Whitted MD, MPH
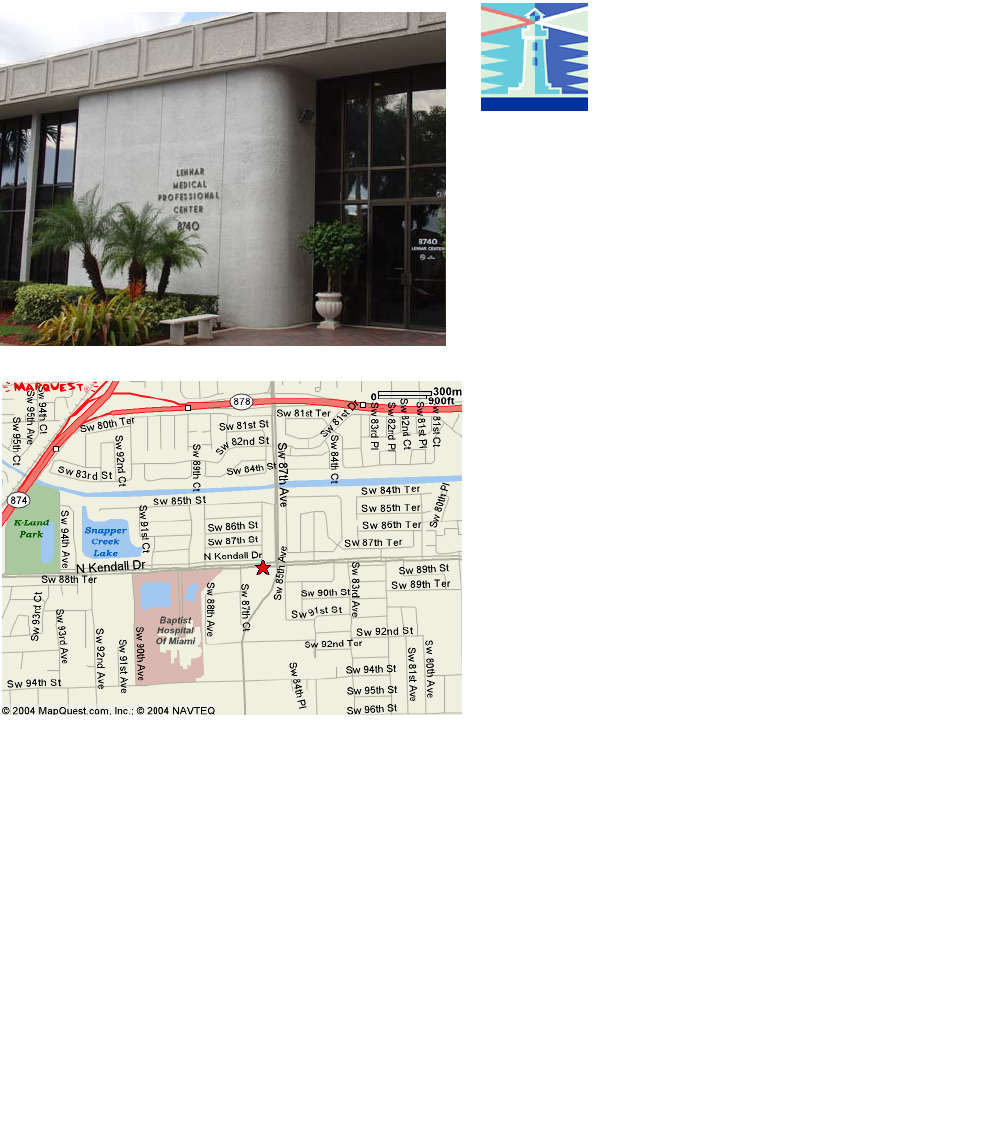
8740 North Kendall Dr.
Suite 101
Miami, Florida 33176-2212
Phone: 305-596-3744
Fax: 305-596-3676
www.drwhitted.net
Raymond Wayne Whitted MD,
MPH
...dedicated to healthy lifestyles and safe, state-of-the-art
surgery for women of all ages.
Endometriosis
Www.4woman.gov; www.endometriosisassn.org
Endometriosis is a common disease that can affect
any menstruating woman from the time of her first
period to menopause. Sometimes, the disease can
last after menopause. There is no cure for endo-
metriosis and it can be hard for a health care pro-
vider to figure out if a woman has it. It can also be
hard to figure out the best way to treat it if a
woman has the disease. Endometriosis can affect
a woman in many ways, such as her ability to work
and have children, and her relationships with her
partner, children, friends, and co-workers. Re-
searchers are working to find out both causes and
ways to manage this disease, so that women who
have it can lead full lives.
What is Endometriosis?
When a woman has endometriosis, the tissue that
lines her uterus, called the endometrium, grows
outside of the uterus. No one is sure why this hap-
pens. This ectopic tissue is mostly found in the
pelvic cavity, usually in one or more places: on or
under the ovaries, behind the uterus, on the liga-
ments that hold the uterus in place, or on the bow-
els or bladder. In extremely rare cases, endome-
triosis can grow in the lungs or other parts of the
body.
Endometriosis is microscopic in its early phase.
As it grows it can create ovarian cysts and perito-
neal implants. These are benign most often and
can cause mild-severe pain, infertility (inability to
become pregnant), and heavy periods.
When a woman has endometriosis, the implants
(which are like the lining of the uterus) can bleed
just like the lining bleeds during a period. This
blood creates inflammation and scar tissue wher-
ever endometriosis is implanted.
Dr. Whitted is dedicated to safe, state-of-the-art,
innovative surgeries and healthy lifestyles for
women of all ages. In a nurturing environment,
the physicians and staff strive to promote a part-
nership in your healthcare and make every effort
to bridge the sterile science of diseases with your
emotional, physical, and spiritual needs. Every-
one is confronted with difficult healthcare deci-
sions at one time or another. You’ll want your
physician and staff to have the knowledge, experi-
ence, and sensitivity to guide you safely through
the decision-making process.
Dr. Whitted provides comprehensive gynecologic
office and surgical healthcare. He is certified in
laparoscopy and hysteroscopy and is an expert in
advanced gynecologic surgery. He has been a
national speaker, trainer, and researcher in ad-
vanced surgical techniques. In addition, Doctor
Whitted is a Certified Menopause Clinician who
educates, trains, and has done research in the
science of menopause. Finally, he is certified in
advanced colposcopy.
Doctor Whitted offers expert education and care in
the following areas:
If you need surgery, Dr. Whitted usually performs
minimally invasive surgery (Vaginal, laparoscopy
and hysteroscopy) and has 21 years experience in
these areas.
Abnormal Paps (HPV) Loss of Urine
Abnormal Menstrual Cycles Menopause
Bladder Prolapse Ovarian cysts
Chronic Pelvic Pain Osteoporosis
Endometriosis Rectocele
Ectopic Pregnancy Uterine Prolapse
Family Planning Vaginal Prolapse
Fibroids (Leiomyoma) Well-Woman Visits
***Evaluation and Diagnosis of Gynecologic Cancers

What are the symptoms of endometriosis?
A common symptom of endometriosis is pain, mostly in
the abdomen, lower back, and pelvic areas. The
amount of pain a woman feels is not associated with
the extent of endometriosis. Some women have no
pain even though their disease affects large areas, or
there is significant scarring. Some women, on the
other hand, have severe pain even though they have
only a few small areas of visible endometriosis.
General Symptoms can include (but are not limited
to):
Extremely painful (or disabling) menstrual
cramps; pain may get worse over time
Chronic pelvic pain (includes lower back pain
and pelvic pain)
Pain during sex (dyspareunia)
Intestinal pain
Painful bowel movements or painful urination
during menstrual periods
Heavy menstrual periods
Premenstrual spotting or bleeding between pe-
riods
Infertility (can’t get pregnant)
Endometriosis can, also, be associated with Irrita-
ble Bowel Syndrome and Interstitial Cystitis.
How is Endometriosis Diagnosed?
A History and Physical exam performed by a knowl-
edgeable Gynecologist is important. Your doctor may
then recommend an ultrasound and possibly an MRI.
These are tests often performed by a Radiologist.
The only way to know for sure, however, is to have
laparoscopy. This surgery is performed with general
anesthesia and involves inserting a telescope through
you belly button. Usually endometriosis can be diag-
nosed (with a biopsy) and treated in the same laparo-
scopic surgery.
What causes endometriosis?
No one knows for sure what causes this disease.
The two plausible theories include retrograde men-
strual flow (menses backs up through the fallopian
tubes into the abdomen) and genetics. Clearly endo-
metriosis “runs in families”.
Researchers, also, are looking at the role of the im-
mune system and how it either stimulates or reacts to
endometriosis. It may be that a woman’s immune
system does not remove the menstrual fluid in the
pelvic cavity properly, or the chemicals made by en-
dometriosis may irritate or promote growth of more
areas. Women who have endometriosis are more
likely to have other auto-immune diseases such as
fibromyalgia, eczema, etc.
Other research is focusing on hormonal impact on
endometriosis. Still further research is looking at
chemical markers. This could help diagnose endo-
metriosis without surgery. In addition, it would allow a
doctor to follow the success of treatments.
What is the treatment for endometriosis?
There is no cure for endometriosis (it is a chronic dis-
ease). But there are many treatments, each of which
has pros and cons. It is important to build a good
relationship with your doctor, so you can decide what
option is best for you.
Pain medication: For some women with mild
symptoms, no further treatment other than medi-
cation for pain may be needed. For women with
minimal endometriosis who want to become preg-
nant, doctors are saying that, depending on the
age of the woman and her amount of pain from
the disease, the best thing to do is to have a trial
period of unprotected sex for six months to one
year. Further treatment may be necessary if
pregnancy doesn’t occur.
Hormone Treatment: There are several hor-
mones used for treatment including BCP (birth
control pills), progesterone pills, Danazol (a weak
male hormone), GnRH agonist (gonadotropin
releasing hormone.
...
dedicated to healthy lifestyles and safe, state-of-the-art, innovative surgery for women of all ages
Birth Control Pills: Usually contain two hor-
mones, estrogen and progesterone. BCPs often
control the growth of the tissue that lines the
uterus and in the same way controls endome-
triosis tissue. BCPs can be taken cyclically (you
will have a menstrual cycle) or continuously (you
likely will not have a menstrual cycle). If a
woman can’t take estrogen then she can take
progesterone only pills or Danazol. All medi-
cines have side effects and for these they in-
clude: weight gain, abnormal bleeding, bloating,
blood clots in the legs, and rarely heart attack
and stroke (usually if used in unhealthy women
who smoke).
Danazol has become more popular than pro-
gesterone only because it may improve PMS
and also significantly reduce the menstrual flow.
The side effects may be oily skin, acne, weight
gain, muscle cramps, headaches, dizziness,
and deepening of the voice.
GnRH Agonist: is a once a month or every
three months injection that prevent ovarian hor-
mone production. As a result a woman doesn’t
have a period and therefore the growth of endo-
metriosis is slowed or stopped. These medica-
tions simulate a temporary menopausal state
and can cause hot flushes, insomnia, mood
swings, memory and concentration loss, possi-
ble bone loss. Usually a person stays on this
medication for 6 months. Usually this medicine
controls the pain of endometriosis which recurs
after the medicine is stopped.
Surgery
It is now believed that surgery combined with
medical therapy is the best combination to have
the greatest success in managing endometriosis
and its symptoms. Surgery is most often per-
formed by Laparoscopy. Endometriosis is ex-
cised and sent for pathologic evaluation. Sur-
gery may be conservative in most cases but
sometimes a woman may elect to remove her
uterus, tubes, and ovaries. This, too, can be
done with laparoscopy.
Women with endometriosis often feel sadness,
fear, anger, confusion, and alone. There is sup-
port available. Talk with your provider.
Raymond Wayne Whitted MD, MPH