Phone: 305-596-3744
Fax: 305-596-3676
www.drwhitted.net
Raymond Wayne Whitted MD, MPH
...dedicated to healthy lifestyles and safe, state-of-the-art surgery for
women of all ages.
R. Wayne Whitted MD, MPH
8740 North Kendall Drive
Suite 101
Miami, Florida 33176-2212
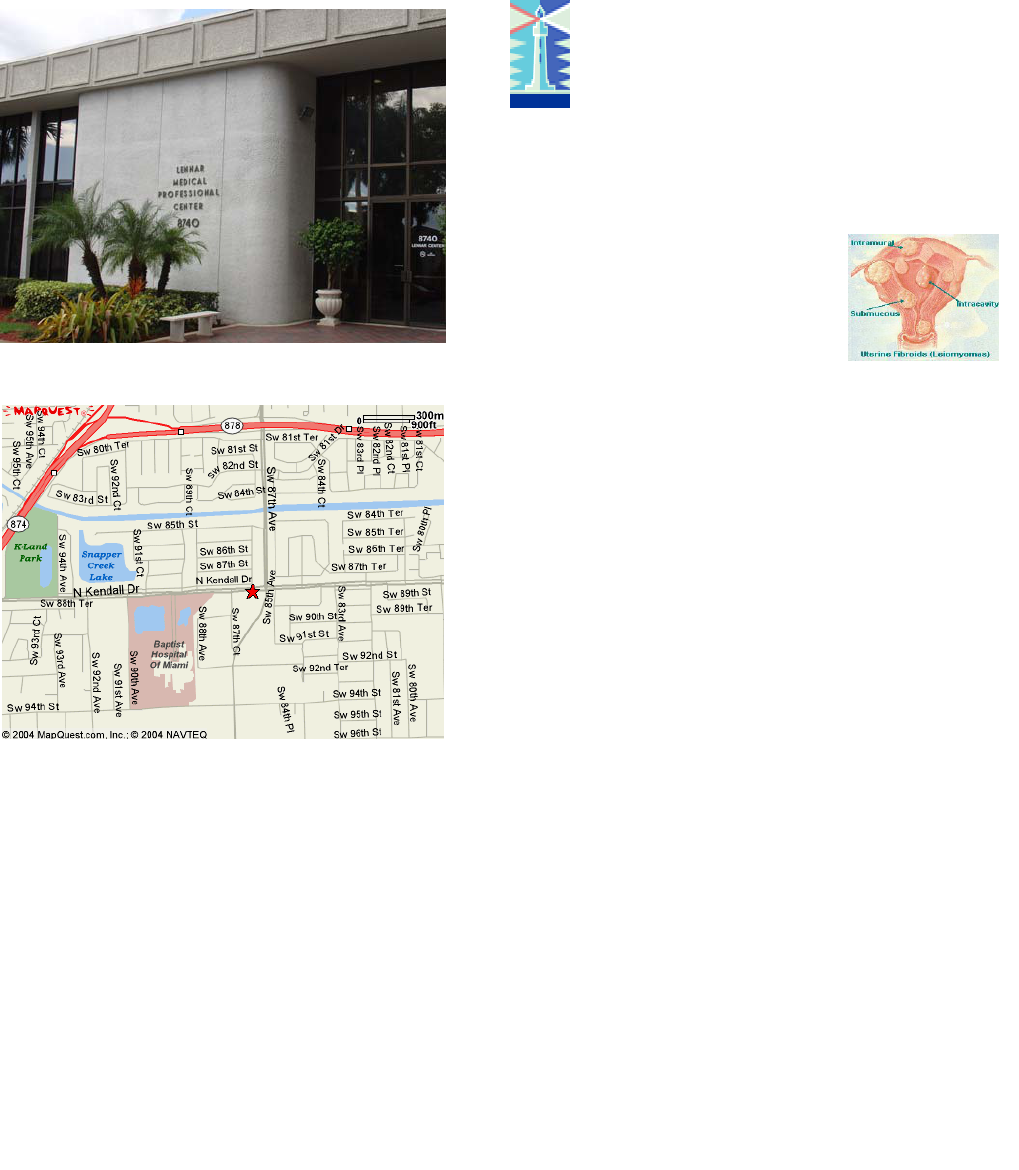
UTERINE “FIBROIDS”
Fibroids (leiomyoma) are muscle
growths in the Uterus that affect
30%-40% of women. They usu-
ally are asymptomatic and can be
left alone and rarely are malignant. Fibroids may
require treatment for the following reasons:
Pain (usually cramping and lower pelvic area)
Bleeding (abnormal)
Urinary frequency and bladder pressure
(usually secondary to size of uterus)
Rapid growth
Fibroids are classified by location. Intra-cavitary
ones are in the uterine lining, intramural are in the
muscle of the uterus, and serosal are on the out-
side of the uterus. Submucosal fibroids are
partly in the lining and muscle. Pedunculated
ones are on the outside of the uterus dangling from
a stalk.
Fibroids are initially diagnosed through pelvic exam
and ultrasound. Office hysteroscopy or saline infu-
sion sonography define intracavitary and submuco-
sal ones. Occasionally an MRI is performed to lo-
cate each individual fibroid within the uterus. This
is especially important in certain types of fibroids if
the hysteroscopic or laparoscopic surgery is con-
sidered.
Dr. Whitted is dedicated to safe, state-of-the-art,
innovative surgeries and healthy lifestyles for
women of all ages. In a nurturing environment,
the physicians and staff strive to promote a part-
nership in your healthcare and make every effort
to bridge the sterile science of diseases with your
emotional, physical, and spiritual needs. Every-
one is confronted with difficult healthcare deci-
sions at one time or another. You’ll want your
physician and staff to have the knowledge, experi-
ence, and sensitivity to guide you safely through
the decision-making process.
Dr. Whitted provides comprehensive gynecologic
office and surgical healthcare. He is certified in
laparoscopy and hysteroscopy and is an expert in
advanced gynecologic surgery. He has been a
national speaker, trainer, and researcher in ad-
vanced surgical techniques. In addition, Doctor
Whitted is a Certified Menopause Clinician who
educates, trains, and has done research in the
science of menopause. Finally, he is certified in
advanced colposcopy.
Doctor Whitted offers expert education and care in
the following areas:
If you need surgery, Dr. Whitted usually performs
minimally invasive surgery (Vaginal, laparoscopy
and hysteroscopy) and has many years experi-
ence in these areas.
Abnormal Paps (HPV) Loss of Urine
Abnormal Menstrual Cycles Menopause
Bladder Prolapse Ovarian cysts
Chronic Pelvic Pain Osteoporosis
Endometriosis Rectocele
Ectopic Pregnancy Uterine Prolapse
Family Planning Vaginal Prolapse
Fibroids (Leiomyoma) Well-Woman visit
***Evaluation and Diagnosis of Gynecologic Cancers

...
dedicated to healthy lifestyles and safe, state-of-the-art, innovative surgery for women of all ages
Hysteroscopic Myomectomy
Laparoscopic Myomectomy Abdominal Myomectomy
If you and your Doctor decide surgery is your best
choice for the management of your fibroids you
will need to understand the 3 approaches to non-
hysterectomy surgical fibroid management.
These are Hysteroscopy, Laparoscopy, and/or
Laparotomy (abdominal incision) approaches..
During Hysteroscopy a telescope is inserted in-
side the uterus through the vagina. No incisions
are used. Distending fluid medium allows for visu-
alization of the intra-uterine abnormalities. Instru-
ments are inserted through the hysteroscope so
that specific abnormalities can be removed. Com-
mon gynecologic problems that can be addressed
with the hysteroscope include:
Removal of Fibroids and Polyps
Endometrial Sampling
Endometrial Ablation (destruction of the endo-
metrial lining)
Adhesiolysis
Septolysis
Fallopian tube cannulization
Removal of an IUD (intra-uterine contracep-
tive device)
The risks associated with hysteroscopy include
bleeding, infection, perforation, injuring abdominal
organs, fluid overload, inability to complete the
procedure, failure to correct the symptoms, and air
emboli.
Hysteroscopy is usually an outpatient surgery and
has minimal postoperative recovery associated
with it.
Laparoscopic Myomectomy is chosen based on
feasibility. It is performed like abdomoinal myo-
mectomy only through minimal incisions on the
abdomen. It is most feasible when there are no
more than 3 fibroids, the largest one measuring no
more than 10cm, and none in the extremely ante-
rior or posterior position. Finally, special surgical
skill is required to perform laparoscopic myomec-
tomy.
When laparoscopic myomectomy is chosen a
“telescope” is placed through the “belly button”
after an incision is made. 3 other small incisions
are made based on the locations of the “fibroids”.
These are usually in the right and left lower quad-
rants and in the suprapubic area.
Once the trocars are placed, instruments are in-
serted through the trocars and the operation is
performed. An injection of diluted pitressin (a he-
mostatic agent) is made in the capsule of the fi-
broid. Once blanching is seen an incision is made
through the capsule identifying the fibroid. It is
then shelled out of its “bed”. The defect in the
uterus is then closed with sutures. The fibroid is
then brought out through one of the trocar sites by
morcellating (cutting into pieces) it. The tissue is
sent for pathologic evaluation.
The risks associated with any myomectomy are
bleeding, infection, injury to abdominal organs,
possible need for cesarean section, possible hys-
terectomy, fibroid recurrence (30%), endometrio-
sis, adenomyosis,
Laparoscopic myomectomy is usually an outpa-
tient surgery and has minimal postoperative re-
covery associated with it.
Abdominal Myomectomy is chosen when the mini-
mally invasive approaches are not feasible. This
method requires a large incision on the abdomen.
The incision can be a “bikini” cut or may need to
be a vertical one (from pubic bone to “belly but-
ton”) depending on the sizes and locations of the
fibroids.
Abdominal myomectomy can have significant
blood loss because the uterus is a very vascular
organ. To minimize this we utilize a tourniquet to
reduce the vascular supply. In addition we inject
the fibroid with a diluted solution of Pitressin (a
vasoconstrictive agent).
The risks associated with abdominal myomectomy
include bleeding, infection, injury to abdominal
organs, possible need for cesarean section, possi-
ble hysterectomy, fibroid recurrence (30%), endo-
metirosis, adenomyosis.
Abdominal myomectomy usually requires a 1 or 2
day hospital stay and requires 3-6 weeks recov-
ery.
Fibroid Location
Fibroid Removal Incision closure
Capsule incision