
The Association of Minimally Invasive Gynecologic Surgeons
…dedicated to safe, state-of-the-art surgery and health life-styles for women of all ages
Local Versus Systemic Therapy
Local therapy is intended to treat a tumor at the site without affecting the rest of the body. Surgery and radiation
therapy are examples of local therapies.
Systemic therapy refers to drugs, which can be given by mouth or directly into the bloodstream to reach cancer
cells that may have spread beyond the breast. Chemotherapy, hormone therapy, and immunotherapy are systemic
therapies.
When patients who have no detectable cancer after surgery are given systemic therapy, it is called adjuvant
therapy. Doctors believe that cancer cells may break away from the primary breast tumor and begin to spread
through the body via the bloodstream even in the early stages of the disease. These cells can't be felt by physical
exam or seen on x-rays or other imaging methods, and they cause no symptoms. But they can establish new
tumors in other organs or the bones. The goal of adjuvant therapy is to kill these hidden cells.
Not every patient needs adjuvant therapy, however. Generally speaking, if the tumor is larger than one-half inch or
the cancer has spread to lymph nodes, it is more likely to have spread through the bloodstream. But there are other
features, some of which have been previously discussed, that may determine whether or not a patient should
receive adjuvant therapy. Recommendations regarding systemic therapy are discussed in the sections on these
treatments and in the section on treatment by stage.
Some patients are given systemic therapy, usually chemotherapy, before surgery to shrink a tumor. This is called
neoadjuvant therapy.
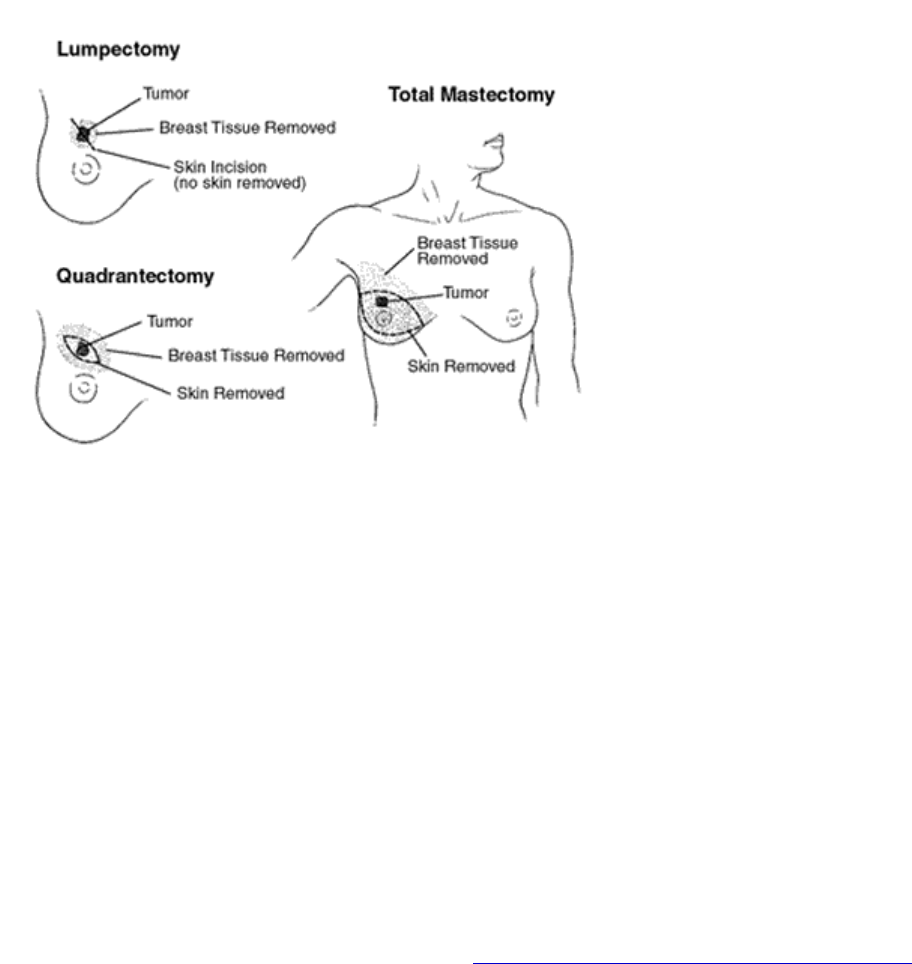
Surgical Procedures for Breast Cancer
Most women with breast cancer have some type of surgery. Operations for local treatment include breast-
conserving surgery, mastectomy, and axillary (armpit) lymph node sampling and removal. In addition, women may
decide to have breast reconstruction at the same time they have the mastectomy, or later on.
Breast conservation therapy: Lumpectomy removes only the breast lump and a surrounding margin of normal
tissue. If examination of the tissue removed by lumpectomy finds there is cancer at the edge of the piece of tissue
removed (margin), the surgeon may need to remove additional tissue. This operation is called a re-excision.
Radiation therapy is usually given at some time after a lumpectomy. If there is to be chemotherapy, the radiation is
usually delayed until the chemotherapy is no longer being given.
Partial or segmental mastectomy or quadrantectomy removes more breast tissue than a lumpectomy (up to one-
quarter of the breast). Radiation therapy is usually given after surgery.
Side effects of these operations include temporary swelling and tenderness and hardness due to scar tissue that
forms in the surgical site.
For most women with stage I or II breast cancer, breast conservation therapy (lumpectomy and radiation therapy) is
as effective as mastectomy. Survival rates of women treated with these 2 approaches are the same. However,
breast conservation therapy is not an option for all women with breast cancer (see section, "
Choosing between
lumpectomy and mastectomy" below.)
Radiation therapy as a part of breast-conserving therapy can sometimes be omitted. Women who may consider
lumpectomy without radiation therapy have all of the following:
age 70 years or older
a tumor 2 cm or less that has been completely removed

a tumor that contains hormone receptors
no lymph node involvement
Mastectomy: In a simple or total mastectomy the surgeon removes the entire breast, including the nipple, but does
Modified radical mastectomy involves the removal of the entire breast and some of the axillary (underarm) lymph
.
Radical mastectomy is an extensive operation removing the entire breast, axillary lymph nodes, and the pectoral
Possible side effects of mastectomy and lumpectomy include wound infection, hematoma (accumulation of blood in
not remove underarm lymph nodes or muscle tissue from beneath the breast. This operation is sometimes used to
treat stage 0 breast cancers.
nodes. This is the most common surgery for women with breast cancer who are having the whole breast removed
(chest wall) muscles under the breast. This surgery was once very common. But because of the disfigurement and
side effects it causes and because modified radical mastectomy has been proven to be as effective as radical
mastectomy, it is rarely done.
the wound), and seroma (accumulation of clear fluid in the wound). If axillary lymph nodes are also removed,
additional side effects may occur, which are described in the section below, "
Axillary lymph node dissection."
Choosing between lumpectomy and mastectomy: The advantage of lumpectomy is that it saves the
y.
ea.
In determining the preference for lumpectomy or mastectomy, be sure to obtain all the facts. Though you may have
rch
than
Although most women and their doctors prefer lumpectomy and radiation therapy, your choice will depend on a
how you feel about losing your breast
therapy
econstruct your breast after having a mastectomy
Lumpectomy or breast conservation therapy is usually not recommended for:
women who have already had radiation therapy to the affected breast
ar apart to be removed through 1
ial lumpectomy along with re-excision has not completely removed the cancer
pecially
nant (risking harm to the fetus)
rapy
Surgical Treatments for Breast Cancer
appearance of the breast. A disadvantage is the need for several weeks of radiation therapy after surger
However, a small percentage of women who have a mastectomy still need radiation therapy to the breast ar
an initial gut feeling for mastectomy to “take it all out as quickly as possible,” the fact is that doing so does not
provide any better chance of long term survival or a better outcome from treatment in most cases. Large resea
studies with thousands of women participating and over 20 years of accumulated information show that when
lumpectomy can be performed, mastectomy does not provide any better chance of survival from breast cancer
lumpectomy. It is because of these facts that most women do not have the breast removed.
number of factors, such as:
how far you have to travel for radiation
whether you are willing to have more surgery to r
your preference for mastectomy as a way to 'get rid of all your cancer as quickly as possible
women with 2 or more areas of cancer in the same breast that are too f
surgical incision
women whose init
women with certain serious connective tissue diseases such as scleroderma, which make them es
sensitive to the side effects of radiation therapy
pregnant women who would require radiation while still preg
women with a tumor larger than 5 cm (2 inches) that doesn't shrink very much with chemothe
women with a cancer that is large relative to a smaller-sized breast
Axillary lymph node dissection: To determine if the breast cancer has spread to axillary (underarm) lymph
nodes, some of these lymph nodes are removed (in an operation called axillary dissection) and examined under the
microscope.
As noted previously, axillary lymph node dissection is part of a radical or modified radical mastectomy procedure
and is usually combined with a breast-conserving procedure such as lumpectomy. Anywhere from about 10 to 40
lymph nodes are removed during axillary lymph node dissection.
Whether or not cancer cells are present in the lymph nodes under the arm is an important factor in selecting
adjuvant therapy. It was once believed that removing as many lymph nodes as possible would reduce the risk of
spread to other parts of the body and improve the chance of curing the cancer.
It is now known that breast cancer cells that have spread beyond the breast and axillary lymph nodes are best
treated by systemic therapy. Axillary dissection is used as a test to help guide other breast cancer treatment
decisions.
The main side effect of removing axillary lymph nodes is lymphedema (swelling of the arm). About 10% to 30% of
women who have underarm lymph nodes removed develop lymphedema. Ways to help prevent or reduce the
effects of lymphedema are discussed in the section, "
What Happens After Treatment for Breast Cancer?". If your
arm is swollen, tight, or painful after lymph node surgery, be sure to tell someone on your cancer care team
promptly.
You may also have temporary or permanent limitations in arm and shoulder movement after surgery. Numbness of
the upper inner arm skin is another common side effect because the nerve controlling this skin sensation travels
through the lymph node area.
Sentinel lymph node biopsy (SLNB): Although lymph node dissection is a safe operation and has low rates of
serious side effects, doctors have developed another way of learning if cancer has spread to lymph nodes without
removing all of them first. This procedure is called the sentinel lymph node biopsy.
In this procedure the surgeon finds and removes the "sentinel node" – the first lymph node into which a tumor
drains, and the one most likely to contain cancer cells. The surgeon injects a radioactive substance and/or a blue
dye into the area around the tumor. Lymphatic vessels carry these substances into the sentinel node and provide
the doctor with a "lymph node map." The doctor can either see the blue dye or detect the radioactivity with a Geiger
counter. He or she then removes the node or nodes (often 2 or 3) for examination by the pathologist.
If the sentinel node(s) contains cancer, the surgeon will perform an axillary dissection – removal of more lymph
nodes in the armpit. This may be done at the same time or several days after the original sentinel node biopsy. The
timing of the axillary dissection depends on how easily the cancer can be seen in the lymph node at the time of
surgery. Sometimes it is obvious and other times it will only be found by thorough microscopic study by a
pathologist.
If the sentinel node is cancer-free, the patient will not need more lymph node surgery and can avoid the side effects
of full lymph node surgery, discussed further on (see the section on lymphedema in "
What Happens After
Treatment for Breast Cancer?").
This limited sampling of lymph nodes is not always appropriate. It is most suitable if there is a single tumor less
than 5 cm in the breast, no prior chemotherapy or hormone therapy has been given, and the lymph nodes do not
feel enlarged.
Sentinel lymph node biopsy is a complex technique that requires a great deal of skill. Therefore, doctors
recommend that sentinel lymph node biopsy be done only by a team known to have experience with this technique.
If you are considering having such a biopsy, ask your health care team if this is something they do regularly.
Reconstructive surgery and breast implant surgery: These procedures are not done to treat cancer but to
restore the breast's appearance after mastectomy. If you are going to have a mastectomy and are thinking about
having reconstruction immediately, it's important to consult with a plastic surgeon who is an expert in breast
reconstruction before the surgery.
Decisions about the type of reconstruction and when it will be done depend on each woman's medical situation and
personal preferences. Your breast can be reconstructed at the same time as the mastectomy (immediate
reconstruction) or at a later time (delayed reconstruction). Reconstruction may use implants and/or tissue from
other parts of your body (autologous tissue reconstruction).
See the American Cancer Society document, "
Breast Reconstruction After Mastectomy" for more information. You
may also find it helpful to talk with a woman who has had the type of reconstruction you are considering. Our Reach
to Recovery volunteers can help you.
What to Expect With Surgery
For many, the thought of surgery can be very frightening. But with a better understanding of what to expect before,
during, and after the operation, many fears can be relieved.
Before surgery: Today, the common procedure for biopsy lets you find out if you have breast cancer within a few
days of your biopsy, but the extent of the breast cancer will not be known until after the surgery for local treatment.
You usually meet with your surgeon a few days before the operation to discuss the procedure. This is a good time
to ask specific questions about the surgery and review potential risks. You will be asked to sign a consent form,
giving the doctor permission to perform the surgery. Take your time and review the form carefully to be certain that
you understand what you are signing.
Sometimes, doctors send material for you to review in advance of your appointment, so you will have plenty of time
to read it and won't feel rushed. You may also be asked to give consent for researchers to use any tissue or blood
that is not needed for diagnostic purposes. Although this may not be of direct use to you, it may be very helpful to
women in the future.
You may be asked to donate blood before some operations, such as a mastectomy combined with natural tissue
reconstruction, if the doctors think a transfusion might be needed. You might feel more secure knowing that if a
transfusion is needed, you will receive your own blood. If you do not receive your own blood, it is important you
know that in the United States, blood transfusion from another person is nearly as safe as receiving your own
blood. Ask your doctor about your possible need for a blood transfusion.
Your doctor will review your medical records and ask you about any medicines you are taking. This is to be sure
that you are not taking anything that will interfere with the surgery. For example, if you are taking a blood-thinning
medicine (even aspirin), you may be asked to stop taking the drug about a week or two before the surgery. Usually,
you will be told not to eat or drink anything for 8 to 12 hours before the surgery, especially if you are going to have
general anesthesia (will be "asleep" during surgery).
You will also meet with the anesthesiologist or nurse anesthetist, the health professional who will be giving you the
anesthesia during your surgery. The type of anesthesia used depends largely on the kind of surgery being done
and your medical history.
General anesthesia is usually given whenever the surgery involves a mastectomy or an axillary node dissection.
You will be given an IV (intravenous) line to give medications that may be needed during the surgery. Usually you
will be hooked up to an electrocardiogram (EKG) machine and have a blood pressure cuff on your arm, so your
heart rhythm and blood pressure can be checked during the surgery.
Surgery: For your surgery, you may be offered the choice of an outpatient procedure or you may be admitted to
the hospital. How long you stay in the hospital depends on the surgery being performed, your overall state of health
and whether you have any other medical problems, how well you do during the surgery, and how you feel after the
surgery. Decisions about the length of your stay should be made by you and your doctor and not dictated by what
your insurance will pay, but it is important to check your insurance coverage before surgery.
As a general rule, women having a mastectomy and/or axillary lymph node dissection stay in the hospital for 1 or 2
nights and then go home. However, some women may be placed in a 23-hour, short-stay observation unit before
going home. In this situation, care is continued at home with a home care nurse visiting you to monitor and provide
care.
Lumpectomy and sentinel lymph node biopsy are usually done in an outpatient surgery center, and an overnight
stay in the hospital is usually not necessary.
The length of the operation depends on the type of surgery being done. For example, a mastectomy with axillary
lymph node dissection will take from 2 to 3 hours. After your surgery, you will be taken to the recovery room, where
you will stay until you are awake and your condition and vital signs (blood pressure, pulse, and breathing) are
stable.
After surgery: You will have a dressing (bandage) over the surgery site. You may have one or more drains (plastic
or rubber tubes) from the breast or underarm area to remove blood and lymph fluid that collects during the healing
process. Care of the drains includes emptying and measuring the fluid and identifying problems the doctor or nurse
needs to know about. Most drains stay in place for 1 or 2 weeks. When drainage has decreased to about 30 cc (1
fluid ounce) each day, often the drain will be removed.
Doctors rarely put the arm in a sling to hold it in place. Most doctors will want you to start moving the arm so that it
won’t get stiff. Women who have a lumpectomy or mastectomy are surprised by how little pain they have in the
breast area. But they are less happy with the strange sensations (numbness, pinching/pulling feeling) in the
underarm area.
Care of the surgery site and arm should be discussed with your doctor. Written instructions about care after surgery
are usually given to you and your caregivers. These instructions should include:
the care of the surgical wound and dressing
how to monitor drainage and take care of the drains
how to recognize signs of infection
when to call the doctor or nurse
when to begin using the arm and how to do arm exercises to prevent stiffness

when to resume wearing a bra
when to begin using a prosthesis and what type to use (after mastectomy)
what to eat and not to eat
use of medications, including pain medicines
any restrictions of activity
what to expect regarding sensations or numbness in the breast and arm
what to expect regarding feelings about body image
a follow-up appointment and referral to a Reach to Recovery volunteer. Through our Reach to Recovery
program, a specially trained volunteer who has had breast cancer can provide information, comfort, and
support. (See the American Cancer Society document, "
Reach to Recovery" for more information.)
Most patients see their doctor within 7 to 14 days following the surgery. Your doctor should explain the results of
your pathology report and talk to you about the need for further treatment. If you will need more treatment, you will
be referred to a medical oncologist and/or radiation oncologist.
Chemotherapy
Chemotherapy is treatment with anticancer drugs that may be given intravenously (injected into a vein) or by
mouth. The drugs travel through the bloodstream to reach cancer cells in most parts of the body. When used as
adjuvant therapy after breast conservation therapy or mastectomy, chemotherapy reduces the risk of breast cancer
recurrence. The chemotherapy is given in cycles, with each period of treatment followed by a recovery period. The
usual course of chemotherapy lasts between 3 to 6 months.
Chemotherapy can also be used as the main treatment for women whose cancer has already spread outside the
breast and underarm area at the time it is diagnosed or spreads after initial treatments. The length of these
treatments is not definite, but depends on how much, if at all, the cancer shrinks.
Chemotherapy given before surgery is called neoadjuvant therapy. The major benefit of neoadjuvant chemotherapy
is that it can shrink large cancers so that they are small enough to be removed by lumpectomy instead of
mastectomy. Another possible advantage of neoadjuvant chemotherapy is that doctors can see how the cancer
responds to chemotherapy. If the tumor does not shrink, then different chemotherapy drugs may be substituted. So
far, there is no evidence, however, that this improves survival.
In most cases, chemotherapy is most effective as an adjuvant therapy, when combinations of more than one
chemotherapy drug are used together. Clinical research studies over the last 30 years have determined which
combinations of chemotherapy drugs are most effective. However, the “best” combination may not have yet been
discovered, so there continue to be clinical research studies comparing one of today’s most effective treatments
against something that may be better.
The most commonly used combinations are:
Cyclophosphamide (Cytoxan), methotrexate (Amethopterin, Mexate, Folex), and fluorouracil (Fluorouracil,
5-FU, Adrucil) [abbreviated CMF]
Cyclophosphamide, doxorubicin (Adriamycin), and fluorouracil [abbreviated CAF]
Doxorubicin (Adriamycin) and cyclophosphamide [abbreviated AC]
Doxorubicin (Adriamycin) and cyclophosphamide followed by paclitaxel (Taxol) T) or docetaxel concurrent
with AC→or docetaxel (Taxotere) (abbreviated AC (abbreviated TAC)
Doxorubicin (Adriamycin), followed by CMF
Cyclophosphamide, epirubicin (Ellence), and fluorouracil with or without docetaxel
Other chemotherapy drugs used for treating women with advanced breast cancer include vinorelbine (Navelbine),
gemcitabine (Gemzar), and capecitabine (Xeloda).
Doctors give chemotherapy in cycles, with each period of treatment followed by a rest period. The chemotherapy is
given on the first day of each cycle, and then the body is given time to recover from the effects of chemotherapy.
The chemotherapy drugs are then repeated to start the next “cycle.” The time between giving the chemotherapy
drugs is generally every 2 weeks, or every 3 weeks. Some drugs are given more often. These cycles generally last
for a total time of 3 to 6 months when given as adjuvant therapy, depending on the drugs used.
The side effects of chemotherapy depend on the type of drugs, the amount taken, and the length of treatment.
Temporary side effects might include fatigue, nausea and vomiting, loss of appetite, hair loss, and mouth sores.
Changes in the menstrual cycle may be temporary or permanent. Because chemotherapy can damage the blood-
producing cells of the bone marrow, patients may have low blood cell counts. This can result in an increased
chance of infection (due to a shortage of white blood cells), bleeding or bruising after minor cuts or injuries (due to a
shortage of blood platelets), and fatigue (due to low red blood cell counts).
There are very effective remedies for many of the temporary side effects of chemotherapy. For example, there are
several drugs that can prevent or reduce nausea and vomiting. A group of drugs called growth factors can help the
patient's bone marrow recover after chemotherapy and can treat problems caused by low blood counts.
Premature menopause (not having any more menstrual periods) and infertility (not being able to become pregnant)
are potential permanent complications of chemotherapy. The older a woman is when she receives chemotherapy,
the more likely it is that she will become infertile or menopausal as a result. This can also lead to rapid bone loss
from osteoporosis.
Adriamycin (doxorubicin) may cause permanent heart damage if used for a long time or in high doses, but doctors
carefully control the dose of this drug. They use echocardiograms and other heart tests in order to monitor the heart
and will stop the medication at the first sign of damage.
Another side effect of chemotherapy is "chemo brain." Many women who have received chemotherapy for breast
cancer will experience a slight decrease in mental functioning. There may be some difficulty in concentration and
memory. This may last a long time, but it rarely interferes with a woman’s ability to do intellectual tasks.
Very rarely, 1 to 2 years after treatment for breast cancer, certain chemotherapy drugs may cause acute myeloid
leukemia, a life-threatening cancer of white blood cells. Chemotherapy's benefits in preventing many breast
cancers from coming back and in saving lives from breast cancer far exceed the risk of this serious but rare
complication.
Finally, many women do not feel as healthy after receiving chemotherapy as they did before. There is often a
feeling of bodily pain and a mild loss of physical functioning. This is a very subtle change that is only revealed by
close questioning of women who have undergone chemotherapy.
Radiation Therapy
Radiation therapy is treatment with high-energy rays or particles that destroy cancer cells. This treatment may be
used to destroy cancer cells that remain in the breast, chest wall, or underarm area after surgery.
In some cases, the area treated by radiation therapy may also include supraclavicular lymph nodes (nodes above
the collarbone) and internal mammary lymph nodes (nodes beneath the sternum ["breast bone"] in the center of the
chest). When given after surgery, radiation therapy is usually not started until the tissues have been able to heal for
about a month. Radiation therapy is usually delayed until chemotherapy is complete.
External beam radiation: This is the usual type of radiation therapy for women with breast cancer. The radiation is
focused from a source outside the body on the area affected by the cancer. This usually includes the whole breast
and, depending on the size and extent of the cancer, may include the chest wall and underarm area as well.
Radiation therapy is much like getting a diagnostic x-ray, but the radiation is more intense. The procedure itself is
painless.
Before your treatments start, the radiation team carefully takes measurements to determine the correct angles for
aiming the radiation beams and the proper dose of radiation. They will make some ink marks or small tattoos on
your skin that they will use later as a guide to focus the radiation on the right area. Patients who receive breast
radiation after lumpectomy are usually treated 5 days a week in an outpatient center for about 6 weeks, with each
treatment lasting a few minutes.

A
new technique to give radiation over a much shorter period of time (5 days total) and to only the part of the breast
with the cancer is currently undergoing clinical research trials. This is called partial breast irradiation. It is hoped
that partial breast irradiation will prove to be equal to the current standard whole breast irradiation. However, partial
breast irradiation is still experimental. Women are encouraged to participate in the major national clinical trial of
partial breast irradiation that started in 2005 and should ask their doctor about this.
One method being used is called Mammosite. It consists of a balloon attached to a thin tube. The balloon is
inserted into the lumpectomy space and filled with a salt water solution. A source of radioactivity is then temporarily
placed into the balloon through the tube. The radioactive material is inserted and removed twice daily for 5 days.
The balloon is then deflated and removed.
Deodorants and antiperspirants can interfere with external beam radiation therapy of the underarm area, so you
should avoid using them until treatments are complete.
The main side effects of external beam radiation therapy are swelling and heaviness in the breast, sunburn-like skin
changes in the treated area, and fatigue. You should avoid exposing the treated skin to the sun because it can
make the skin changes worse. These changes to the breast tissue and skin usually go away in 6 to 12 months.
A rare complication is the development of another cancer called angiosarcoma. In one group of 20,000 patients, 9
patients developed this cancer about 4 to 8 years after post-lumpectomy radiation. It is treated with mastectomy but
can be fatal. For more information see the American Cancer Society document, "
Sarcoma – Adult Soft Tissue
Cancer."
In some women, the breast becomes smaller and firmer after radiation therapy. Radiation therapy of axillary lymph
nodes also can cause lymphedema. (This is discussed in the section, "
"What Happens After Treatment for Breast
Cancer?".) Radiation therapy is not given during pregnancy because it can harm a fetus.
Brachytherapy: Brachytherapy, also known as internal radiation, is another way to deliver radiation therapy.
Instead of aiming radiation beams from outside the body, radioactive seeds or pellets are placed directly into the
breast tissue next to the cancer. Often this is used to add an extra "boost" of radiation to the tumor site. This
method is also being studied in clinical trials as the only source of radiation for women who have had lumpectomy.
So far the results have been promising, but more experience is needed with this technique before it can be
recommended as standard treatment.
Hormone Therapy
The hormone estrogen is produced mainly by a woman's ovaries until menopause, and then by conversion of a
testosterone-like hormone made by the adrenal gland, which is then converted into estrogen mostly in the body’s
fat tissue. Estrogen promotes the growth of about two thirds of breast cancers (those containing estrogen or
progesterone receptors). Because of this, several approaches to blocking the effect of estrogen or lowering
estrogen levels are used to treat breast cancer.
Tamoxifen: The antiestrogen drug that has been used most often is tamoxifen (Nolvadex). It is taken daily in pill
form. Taking tamoxifen after surgery, usually for 5 years, reduces the chances of the cancer coming back by about
50% for women with early breast cancer if the cancer contained estrogen or progesterone receptors. Tamoxifen is
also used to treat metastatic breast cancer. It is used to prevent the development of breast cancer in a woman at
high risk, as well.
Tamoxifen can increase the risk of developing cancer of the lining of the uterus (endometrial cancer). This cancer is
usually diagnosed at a very early stage and is generally curable by surgery. Tamoxifen can also increase the risk of
uterine sarcoma, a rare cancer of the connective tissue of the uterus. If you are taking tamoxifen, tell your doctor
right away about any unusual vaginal bleeding (a common symptom of both of these cancers). Most uterine
bleeding is not due to cancer, but this symptom always needs prompt evaluation.
Blood clots are another serious side effect of tamoxifen. Other side effects of tamoxifen may include weight gain
(although recent studies have not found this), hot flashes, vaginal discharge, and mood swings. Early cataracts
may occur rarely. Nonetheless, for most women with breast cancer, the benefits of taking tamoxifen far outweigh
the risks.
Some patients whose cancer has spread to their bones may experience a "tumor flare" with pain and inflammation
in the muscles and bones when treated with tamoxifen. It usually subsides quickly. However, the patient may also
develop a high calcium level in the blood that cannot be controlled. If this occurs, the treatment may need to be
stopped.
Aromatase inhibitors: Three drugs that stop estrogen production in postmenopausal women have been approved
for use in treating both early and advanced breast cancer. These drugs are called letrozole (Femara), anastrozole
(Arimidex), and exemestane (Aromasin). They work by blocking an enzyme responsible for producing small
amounts of estrogen in postmenopausal women. They cannot stop the ovaries of premenopausal women from
producing estrogen. For this reason they are only effective in postmenopausal women.
These drugs have been compared with tamoxifen as adjuvant hormone therapy in postmenopausal women with
early breast cancer. Clinical trials have been performed comparing tamoxifen with one of the aromatase inhibitors
“head to head” for a total of 5 years, or after either 2 years or 5 years of tamoxifen. In each of these studies there
has been a clear advantage to using either the aromatase inhibitor instead of tamoxifen for a total of 5 years or
following several years of tamoxifen rather than keeping women on tamoxifen for 5 years as their only hormone
therapy. Clinical trials continue to be done to try and figure out which of these strategies is the best. The aromatase
inhibitors have fewer side effects than tamoxifen because they don’t cause endometrial cancer and very rarely
cause blood clots. They can, however, cause osteoporosis and bone fractures because they remove all estrogens
from a postmenopausal woman.
Many doctors prefer aromatase inhibitors over tamoxifen as the first hormonal treatment for postmenopausal
women whose breast cancer has come back, if the cancer is hormone receptor positive.
Raloxifene: Raloxifene (Evista) is a drug that, like tamoxifen, blocks the effect of estrogen on breast tissue and
breast cancer. It was originally developed to treat osteoporosis because it has the same bone strengthening effect
as estrogen. But in other ways it is an antiestrogen. It is currently being tested to see if it can reduce women's risk
of developing breast cancer. Until more testing is done, raloxifene is not recommended as hormonal therapy for
women who have already been diagnosed with breast cancer.
Toremifene: Toremifene (Fareston), another antiestrogen drug closely related to tamoxifen, may be an option for
postmenopausal women with breast cancer that has metastasized. Toremifene is an antiestrogen medicine that is
used in tumors that are estrogen-receptor positive or whose estrogen-receptor status is unknown.
Fulvestrant: Fulvestrant (Faslodex) is a newly approved drug that also acts via the estrogen receptor, but instead
of blocking it, this drug eliminates it. It is often effective even if the breast cancer is no longer responding to
tamoxifen. It is given by injection once a month. Hot flashes, mild nausea, and fatigue are the major side effects. It
is only given to women who are already in menopause.
Ovarian ablation: Removing estrogens from premenopausal women is another effective way of treating breast
cancer in hormone-responsive cancer. This can be done surgically, by removing the ovaries. It also can be done
with drugs called luteinizing hormone-releasing hormone (LHRH) analogs. The usual drugs are goserelin or
leuprolide. These drugs block the mechanism that causes ovaries to make estrogens. They are now being tested
as adjuvant therapies. Chemotherapy drugs may also damage the ovaries of premenopausal women so they no
longer produce estrogen.
Megestrol acetate: Megestrol acetate (Megace) is a progesterone-like drug used for hormone treatment of
advanced breast cancer, usually for women whose cancers do not respond to the other hormone treatments. Its
major side effect is weight gain, and it is sometimes used to reverse weight loss in patients with advanced cancer.
Other ways to control hormones: Androgens (male hormones) may be considered after other hormone
treatments for advanced breast cancer have been tried. Androgens cause masculine characteristics to occur, for
example, more body hair and a deeper voice. They are sometimes effective
Monoclonal Antibody Therapy with
Trastuzumab (Herceptin
®
)
Trastuzumab (Herceptin
®
) is a monoclonal antibody that attaches to a growth- promoting protein known as
HER2/neu, which is present in small amounts on the surface of normal breast cells and most breast cancers. About
one third of breast cancers have too much of this protein and tend to grow and spread more aggressively.
Herceptin can prevent the HER2/neu protein from making breast cancer cells grow and may also stimulate the
immune system to more effectively attack the cancer.
Herceptin can shrink some breast cancer metastases that return after chemotherapy or continue to grow during
chemotherapy. Treatment that combines Herceptin with chemotherapy may be more effective than chemotherapy
alone in some patients.
Recently, clinical trials have been completed that found that adding trastuzumab to chemotherapy lowers the
recurrence rate and death rate over chemotherapy alone after surgery in women with HER2/neu positive early
breast cancers. Using trastuzumab along with chemotherapy may become standard adjuvant treatment for these
women. The clinical trials were presented in May of 2005. More trials are underway to see if these results can be
improved.
Compared with chemotherapy drugs, the side effects of Herceptin are relatively mild. They may include fever and
chills, weakness, nausea, vomiting, cough, diarrhea, and headache. These side effects are usually associated with
the first dose and not seen again. Some women being treated with Herceptin, however, have experienced heart
damage leading to a problem called congestive heart failure. For most women, this effect on the heart has been
temporary and has improved when the drug is stopped. The risk of heart problems is about 3 times higher when
Herceptin is given with anthracyclines, a class of chemotherapy drugs that includes doxorubicin (Adriamycin) and
epirubicin (Ellence) and may not be reversible. Major symptoms are shortness of breath and severe fatigue.
Women experiencing these symptoms should call their doctor right away.