
The Association of Minimally Invasive Gynecologic Surgeons
…dedicated to safe, state-of-the-art surgery and health life-styles for women of all ages
R. Wayne Whitted MD, MPH
Paul A. Pietro MD
Marina Santana MMS, PA
8740 N Kendall Dr. Suite 101
Miami, Florida 33176
Phone: 305-596-3744
Why Incontinence Need Not Be a Problem
Perhaps no medical problem is both as common and as cloaked in secrecy as urinary incontinence —the
involuntary loss of urine. Although it occurs in men and women of all ages (at least 13 million Americans and
50 percent of people over 65) you probably can't remember ever hearing someone talk casually about it. People
who feel comfortable discussing almost any physical complaint, even reproductive difficulties, will probably
never mention a bladder problem. Despite the breakthrough advertising for adult absorbent products, leaking
urine remains a strong cultural taboo, one we learn as young children and carry with us for life.
Unfortunately, this sense of shame inhibits many people with incontinence from seeking help—and that, it turns
out, is a mistake. Although studies show that only one in 12 incontinent people sees a doctor for help, research
also indicates that eight out of 10 could benefit from therapy.
Many people also forgo help under the mistaken impression that incontinence is a normal part of aging,
something that we all must learn to live with. To some extent, the advertising for adult absorbent products,
while helping to bring the subject out in the open, has fostered this misconception. But the truth is that most
incontinence is treatable—and quite often curable. It is not an inevitable part of getting older, and no one need
accept it.
Not a Simple Problem
Incontinence is not a disease, it's a symptom. It means that something isn't working right with your body. There
are two broad categories of incontinence: transient and chronic.
become more susceptible to the effects of some medications on urinary function.
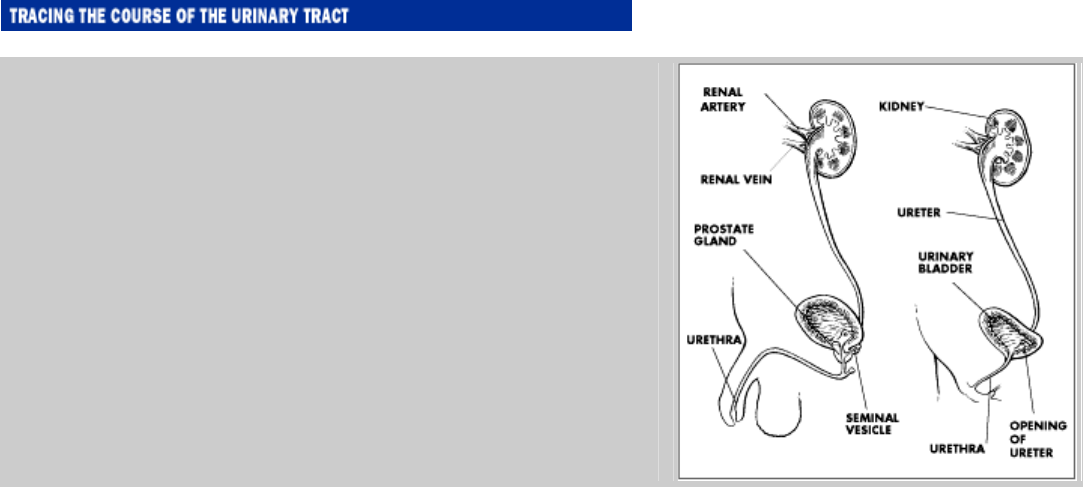
Originating at the kidneys, the urinary tract conducts waste fluid
down the ureters and into the bladder, where it accumulates until
expelled through the urethra. Note the striking difference in the
lengths of the male and female urethras. This, more than any other
factor, accounts for a woman's greater vulnerability to bladder
infections.
How the System Works
Because we learn to use a toilet as young children, we tend to think that controlling urination is simple, and as
adults we take it for granted. But that control is the product of many complex organs working together
perfectly. To achieve it, the urinary system, the pelvic muscles, the spinal cord, and the brain must all be in fully
coordinated working order.
The urinary system comprises the two kidneys, two muscular, tube-like ureters, the bladder, and the urethra.
The kidneys filter wastes from the blood and continuously produce urine, about a quart a day for most people.
The ureters move urine from the kidneys to the bladder, where it is stored until the bladder muscle, called the
detrusor muscle, pushes it out of the body through the urethra. A circular muscle, the sphincter, controls the
opening and closing of the urethra and plays a vital role in continence.
As urine collects in the bladder, the bladder expands, eventually signaling the spinal cord that it is full. When
the signal is strong enough, it enters our awareness and we know it's time to find a toilet. At the right moment,
the spinal cord signals the bladder that it's okay to empty, producing the voiding reflex: the contraction of the
bladder muscle that forces urine out through the urethra.
In most adults, 8 to 10 ounces will collect in the bladder before the brain gets the signal that urination is
necessary. (The normal capacity of the bladder is about 12 to 16 ounces.) The brain is able to suppress the urge
if necessary. When you are in the checkout line at the supermarket, for example, the brain tunes out the
bladder's signal. When you reach a toilet, the brain sends the okay.
How often should urination occur? For most people, every three to four hours, under normal conditions. Health
problems, certain medications, pregnancy, or high fluid intake may make urination more frequent.
Diet, Drugs, and Transient Incontinence
What you eat and drink, as well as the medicines you take, can affect your urinary system. Some cases of
transient incontinence can be improved or eliminated simply by modifying diet or medications.
Foods. Diet rarely causes urinary problems for most people. But for some, certain foods and beverages can be
troublemakers. While there is not a great deal of medical research on the effects of these dietary items, they
remain under suspicion because some people with incontinence have reported them as causing problems.
Possible trouble-makers include:
• Alcoholic drinks, including beer and wine
• Carbonated soft drinks
• Caffeine in coffee, tea, or soft drinks, or in medicines
• Milk and milk products
• Coffee or tea, even when decaffeinated
• Citrus fruit and juices
• Tomatoes and tomato-based products
• Spicy foods
• Sweeteners including sugar, honey, and corn syrup
• Chocolate
• Artificial sweeteners
Drugs. Several types of medicines may affect how the bladder functions. When you talk with your doctor, be
sure to mention all the medications you're taking—for whatever reason. Some seemingly unrelated drug could
be part of the problem. One study, for example, showed that the antihypertensive drug Prazosin (Minipress),
which is also prescribed to treat some types of incontinence, actually produced incontinence in many women
taking it to control blood pressure. Drugs especially likely to be at fault include diuretics, such as those used to
treat high blood pressure; sedatives; pain relievers; antihistamines; cold remedies; antidepressants; drugs that
control spasms, such as those used to treat Parkinson's disease; and certain drugs that affect the involuntary
nervous system, such as phenylpropanolamine (Ornade, Dexatrim), phentolamine (Regitine), prazosin
(Minipress), terazosin (Hytrin), and phenoxybenzamine (Dibenzyline).
Chronic Incontinence: The Seven Types
There are not one, but seven possible forms of chronic incontinence. Doctors classify the condition as stress,
urge, reflex, overflow, functional, mixed, or total.
Stress Incontinence
The classic sign of stress incontinence, also known as sphincter insufficiency, is a tendency to leak urine when
laughing, sneezing, coughing, or lifting. Usually only a small amount of urine escapes. Stress incontinence is fa
r
more common in women than in men.
The problem isn't with the bladder itself, but with the urethra or the pelvic muscles. Often, the urethra doesn't
stay tightly closed because of weakness or damage to the surrounding muscle and tissue. In addition, weakened
pelvic muscles and tissues sometimes can't support the bladder and other organs properly.
In women, a major cause of weakening is damage from pregnancy and childbirth. After menopause (or removal
of the ovaries) a lack of estrogen may also cause the pelvic muscles and urethra to thin and weaken. In men,
stress incontinence, when it does occur, is usually the result of injury to the urethra, sometimes after prostate
surgery. There is also some evidence that being overweight may contribute to the problem.
Urge and Reflex Incontinence
Urge incontinence may be the diagnosis when you feel an urgent need to urinate and rush to the bathroom but
j
ust don't make it there in time. Unlike stress incontinence, this form of the problem originates in the bladder
itself. The voiding reflex slips out of control, the bladder muscle contracts, and urine is forced out even though
the time and place aren't appropriate. The difficulty can be caused by inflammation of the bladder or urethra, or
by disorders of the nervous system, such as spinal cord injury, stroke, Parkinson's disease, dementia, or multiple
sclerosis. In some cases, a cause cannot be identified.
Reflex incontinence is a variant of urge incontinence, in which urine is lost suddenly but, in this case, without
warning. As with urge incontinence, the bladder is contracting and expelling urine at the wrong time and place.
Causes include nervous system problems or bladder tumors.
Overflow Incontinence
This form of the problem is characterized by periodic leakage of small amounts of urine. It occurs when the
bladder cannot empty completely. Even though the bladder may be holding a great deal of urine, someone with
overflow incontinence feels no need to void—and is unaware of voiding when the leakage occurs. The
condition is due either to a failure of the bladder to contract properly or to a partial blockage of the urethra.
If the problem is with the bladder, it usually stems from some difficulty with the nerves that control the bladder,
perhaps due to a spinal cord injury, or nerve damage caused by diabetes. If the culprit is a partial blockage of
the urethra, the most likely cause is an enlarged prostate. While it is normal for this gland, which surrounds the
urethra, to enlarge as a man ages, excessive enlargement can pinch the urethra, making it difficult for urine to
pass.
Blockages in the urethra can also be caused by development of scar tissue following surgery or an accident, or
by a lack of coordination between the bladder and the pelvic muscles (dyssynergia) due to nervous system
problems, spinal cord injury, or multiple sclerosis.
Functional Incontinence
In this type of incontinence, the urinary system is working fine, but the individual is unwilling or unable to get
to the toilet when necessary. Medical problems that make it difficult or painful to move, such as severe arthritis,
balance problems, broken bones or joint problems, muscle weakness, or fatigue may lead to this type of
incontinence. Other causes include dementia or impaired memory.
Mixed and Total Incontinence
In many cases of incontinence, several problems are at work; and these cases are referred to as mixed
incontinence. Typically, there may be both stress and urge incontinence, reflecting disorders in both the urethra
and the bladder.
The rarest of these conditions is total incontinence—the complete loss of control and continual leakage of urine.
This form of incontinence can be caused by a hole in the bladder (fistula), injury to the urethra, or a ureter that
is not in the right place (ectopic ureter).
Cystoceles and Incontinence
Many women have a cystocele, a condition in which the bladder protrudes down into the vagina, like a hernia o
f
the bladder wall. A cystocele can sometimes follow childbirth, or heavy lifting. It can also result when the loss
of estrogen at menopause weakens vaginal tissues. Often a cystocele causes no problems, but in some women it
may make urination difficult. If the cystocele becomes a problem, a pessary may be recommended or surgery
may be required. A pessary is a device, often made of latex, that is placed in the vagina to help hold the pelvic
organs in place. There are many types, but all should be comfortable to wear. A pessary is removed regularly
for cleaning, by either you or your doctor, depending on the style.
Pin-Pointing the Cause
Getting a diagnosis is the first step in treating incontinence. The best place to start is your regular health care
provider, who may be an internist, a general practitioner, or, for many women, a gynecologist. If your doctor is
not experienced in treating incontinence or if you need more help, you may want to see a specialist.
Gynecologists, urologists, and geriatricians are likely to have more experience treating incontinence, or there
may be a continence clinic or specialist in your area. Ask your doctor for a referral or call a university medical
center, hospital, or medical society.
Preparing for Your Appointment
As soon as you make your appointment, start preparing to make the most of it. Experts recommend that you
keep a record of when you go to the bathroom and when you have leakage for at least 4 days before you see the
doctor. What were you doing when the leakage occurred? Note whether an activity such as sneezing, lifting,
changing position, or sex seems to bring on leakage, or whether it is sudden and unexpected. What time of day
or night do the incidents take place? What do you eat and drink each day? Don't change your habits for the
record; you need to know what is really happening. List or bring all your medicines to the appointment,
including any over-the-counter drugs that you take occasionally. Experts recommend bringing the medicines
themselves, so that you and your doctor both know exactly what you are taking.
Before your appointment you should also make a list of questions you want to ask. These might include:
• What is causing the problem? Does the condition have a name?
• Can the condition be treated? How?
• Have you treated many people with this problem? How many improved?
• What are the likely outcomes of possible treatments? Which is the first to try, the second and so on?
• Are any of the medications I'm taking a possible cause?
• Are there any dietary changes I should make?
• Are there exercises that might help me?
• Is surgery ever necessary for this condition?
• Should I see a specialist for this condition?
Be sure you understand the answers before you leave the doctor's office. If you don't feel the doctor is
concerned with finding a cause or hasn't had significant experience treating other people with the problem, see
another doctor. While great strides have recently been made in understanding and treating incontinence, not all
physicians have the same degree of familiarity with the condition. You need to find one who has experience and
up-to-date knowledge.
The Examination
Many people find it embarrassing to discuss urinary problems, and the doctor will understand if you have
difficulty talking about the condition. But your explanations are an important part of the examination, so do the
best you can to put embarrassment aside and explain fully what you mean. Try to be specific. For some people,
"leaking a lot" might mean they feel damp; for others, it might mean a flood. Explain clearly what happens.
The doctor will take or review your medical history, ask you questions about your lifestyle (eating, sleeping,
and sexual habits), your emotional situation, and the incontinence itself. Having your leakage record with you
will help.
Next, the doctor will conduct an exam. Because continence involves not only the urinary system, but also the
nervous system and pelvic muscles, your doctor will usually do an abdominal, rectal, and neurological
examination, as well as a pelvic exam for women.
Possible Tests
While not every doctor does things the same way, there are a few basic tests you might encounter at your first
visit.
The doctor may ask you to cough while lying down and standing up, and to bend, bounce, or walk. This is a
stress test to see whether stress incontinence occurs.
You may be asked for a urine specimen for urinalysis, to check for abnormalities or infection. After you have
urinated, the doctor may check to see if your bladder emptied completely by doing a bladder catheterization. In
this procedure, a sterile tube is passed through your urethra into the bladder to drain any remaining urine.
Bladder catheterization is quick and should not be painful.
The doctor may also order blood tests to check for sugar or calcium and to determine how well your kidneys are
working. For women, a simple cotton swab test in which a long-handled cotton swab is inserted into the urethra
to determine the position of the bladder neck, may be used to see if the urethra has slipped out of normal
position.
Based on your history, interview, leakage record, and these tests, the doctor may be able to prescribe treatment
at this point. However, if more information is needed to make a diagnosis, the doctor may need to order
additional tests. These are not dangerous or particularly painful, but for some people they may be unpleasant,
because they involve private parts of the body and some require urinating while someone else is watching.
Discuss any concerns you may have with the doctor before the tests so you will be as comfortable as possible
during them.
Cystometry measures the pressure in the bladder as it fills. A catheter is inserted through the urethra into the
bladder and the bladder is then filled with sterile water or carbon dioxide. You signal when you feel the bladder
filling and when you feel you must urinate. When the bladder is full, you cough or bear down to see if leakage
occurs, and then urinate. The procedure should not be painful, though there may be discomfort from the
catheter.
Cystoscopy gives the doctor a look at the urethra and bladder by passing a narrow, flexible tube, called a
cystoscope, through the urethra into the bladder. After the cystoscope is in place, the bladder is filled with a
sterile solution. This test may be mildly uncomfortable, and is sometimes done under anesthesia.
Electromyography is a recording, either with a graph or on a screen, that shows pelvic muscle contractions. To
make the recording, electrical sensors are placed on the skin near the anal sphincter and inside the vagina or
urethra, and a small probe may be inserted into the vagina or rectum. The sensors measure electrical activity of
the muscles at rest and when contracting. Discomfort should be minimal.
Manometry uses small balloons to measure the strength of the muscles in the pelvic floor. The balloons are
inserted into the vagina or rectum and then filled with air or water. When you contract the pelvic floor muscles,
the pressure on the balloons is measured. There is little discomfort.
Urethral pressure profilometry measures pressure in the urethra and compares it with bladder pressure. A
catheter is passed through the urethra into the bladder; the bladder is filled with about 3 ounces of water, and
b
ladder pressure is measured. Then the catheter is slowly pulled back through the urethra, measuring pressure at
different points. The test may be repeated while you cough or bear down. There may be mild discomfort.
Uroflowmetry shows how rapidly the bladder empties. With a full bladder, you urinate as usual into a
collecting device with a timer attached.
The instrument determines how long it takes for the stream to start, the amount voided each second,
the strength and smoothness of the stream, and any dripping after urination. There is no discomfort.
Voiding cystourethrography uses x-rays to examine the bladder and urethra. The test includes an x-ray of the
abdomen and pelvis to determine the position of kidneys, ureters, and bladder and to check for abnormalities of
the spine, any masses, impaction, or kidney stones. Then a catheter is passed through the urethra into the
bladder and the bladder is filled with liquid that is visible on an x-ray film. X-rays of the bladder are taken from
several angles. Then you are asked to bear down and finally urinate while x-rays are taken of the urethra. After
urination, another x-ray is taken to check for liquid remaining in the bladder. There may be mild discomfort
from the catheter.
Ultrasound, very high frequency sound waves, can be used to check the shape, size, and location of the
kidneys, ureters, bladder, and prostate. There is no discomfort.
The Options for Treatment
Treating chronic incontinence is not an exact science; nor is there universal agreement on which approaches are
best in each situation. And because not all people react the same way to treatment, you may need to try another
method if the first one you try doesn't work for you.
Experts do agree, however, that the most conservative appropriate treatment should be tried first in all cases.
There are five major types of treatment available: behavioral training, muscle training, medicines, bladder
catheterization, and surgery.
Behavioral Techniques
Biofeedback is used in many medical disorders, including incontinence, to help people become aware of and
gain control of the body's ordinarily involuntary responses. During a biofeedback session, several
measurements, such as heart rate, blood pressure, skin temperature, and bladder pressure, are continually
measured. These measurements are displayed on a screen for you to watch, or sounded as a tone for you to hear.
Using the visible or audible feedback and expert coaching, you can learn to modify your body's responses.
Studies indicate that more than 80 percent of people treated with biofeedback for urge, stress, or mixed
incontinence achieve improvement or a complete cure.
For men and women with urge incontinence, the biofeedback session is similar to cystometry (see above), as
you learn to relax the bladder long enough to reach the toilet. Biofeedback is also used to help people strengthen
and control the pelvic muscles.
Bladder training is often used for urge incontinence, and may be helpful in stress incontinence as well.
Through bladder training, people learn to urinate at regular short intervals, and develop the ability to hold urine
longer without leakage. In one recent study, bladder training techniques put an end to incontinence for 83
percent of the women in the trial. In another study, bladder training reduced the number of incontinent episodes
by 57 percent and the quantity of urine loss by 54 percent.
Muscle Training
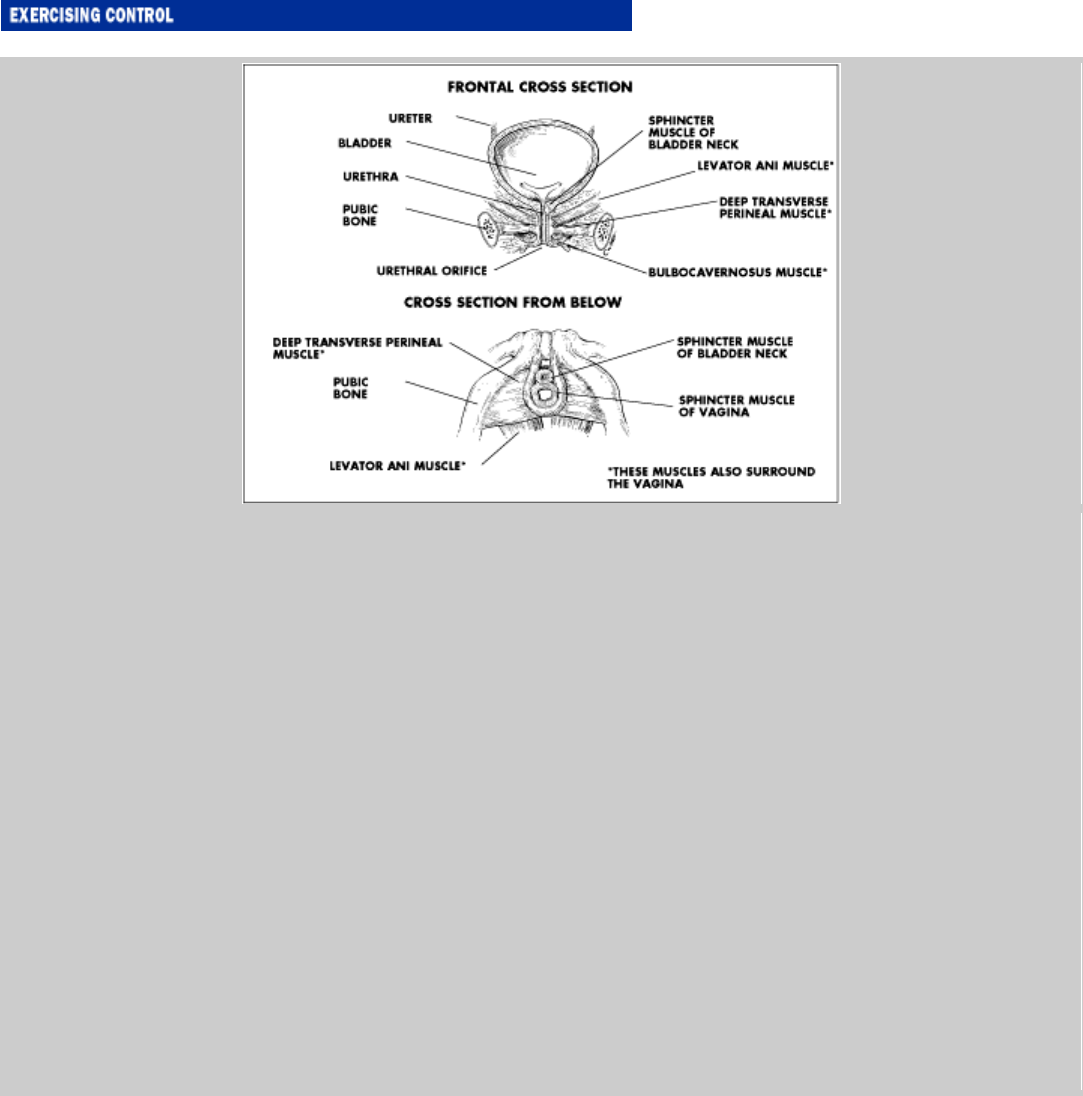
Pelvic muscle exercises, also called Kegel exercises, can help with urge, stress, and mixed incontinence by
strengthening and training the pelvic muscles that control urination. In these exercises, you squeeze and relax
the pelvic muscles for a set number of repetitions each day. (See the box on "Exercising Control.")
Electrical muscle conditioning treatment usually employs a low-voltage electrical device that is placed into
the vagina or rectum to cause sphincter muscle contractions. It is used when the pelvic muscles can't be
controlled voluntarily. The electrical stimulation strengthens the sphincter muscles, allowing better control.
Treatment sessions typically take about 20 minutes every 1 to 4 days. They are especially helpful for stress and
urge incontinence.
Medications
Chronic urge, stress, mixed, and overflow incontinence can be treated with medications that affect the bladder
or the urethral sphincter. Medications for urge incontinence prevent the bladder from contracting. This reduces
the feeling of urgency and decreases the amount of leakage. These medications include: dicyclomine (Bentyl),
flavoxate (Urispas), hyoscyamine sulfate (Anaspaz), imipramine (Tofranil), oxybutynin (Ditropan), tolterodine
(Detrol), and propantheline (Pro-Banthine).
Medications for stress incontinence strengthen the urethral sphincter. These include ephedrine, imipramine
(Tofranil), phenylpropanolamine (Dexatrim), and pseudoephedrine (Sudafed).
To treat mixed incontinence, two drugs may be used together—one to relax the bladder and another to
strengthen the urethral sphincter—or imipramine (Tofranil) may be used alone, since it has both effects. For
women, estrogen (Premarin) is another possibility, since it can help counter the thinning of the vaginal and
urethral tissues that can lead to incontinence.
Overflow incontinence is treated with drugs that stimulate the bladder to contract, such as bethanechol
(Urecholine, Duvoid), or drugs that decrease urethral pressure such as clonidine (Catapres). When blockage of
the urethra from an enlarged prostate is the cause, prazosin (Minipress) or terazosin (Hytrin) may be used to
relax the urethral sphincter.
There are side effects from most of the drugs used to treat incontinence. However, most people find they can
manage the side effects successfully or that they diminish over time. If you find that you do have a problem
with a medication, be sure to talk with your doctor before you stop taking it. He or she may be able to modify
the dosage or treat the side effects sufficiently to allow you to continue.
Surgery
Surgery is the last resort for most incontinence problems, except in cases where a physical obstruction of the
urethra prevents the bladder from emptying, as in prostate enlargement.
For men, in whom the problem is often urge or overflow incontinence due to an enlarged prostate, the most
common surgery is to remove part or all of the offending gland. When part of the prostate is removed, the
operation is called a transurethral resection of the prostate or TURP. If the entire prostate is removed, the
surgery is called a prostatectomy. (For more information about prostate surgery, see Chapter 31).
Unfortunately, the surgery itself sometimes leads to continued incontinence. A short-term problem is common
following prostate surgery, but chronic incontinence occurs about 10 percent of the time. Overflow
incontinence, caused by scar tissue from the surgery or remaining prostate tissue, may require a second
operation. Damage to the urethral sphincter may result in stress or total incontinence. An inflatable artificial
sphincter can cure this kind of incontinence in up to 90 percent of cases, as can periurethral injection, in which
special substances, such as Teflon, collagen (Contigen), or urethrin (Polytef) are injected into the tissues
surrounding the urethra to add bulk and help it close.
The pelvic muscles support the abdominal and pelvic organs, help control bowel and bladder functions, and
facilitate sexual response. If weakened, they will be less effective at all those chores. There is, however, no
reason to accept this situation. You can take action to improve their condition by beginning Kegel exercises—
exercises that work the muscles of the pelvic floor. Make up your mind to learn to love them, because Kegel
exercises are a lifelong project. They must be done regularly forever to maintain good muscle condition.
You perform a Kegel exercise by first squeezing and then relaxing the pelvic floor muscles. Sounds simple, but
for many people, finding the right muscles to squeeze can be a major challenge. One way is to try to stop while
urinating—the muscles you use for this are the ones you want. Another technique is to pretend that you need to
pass gas but must hold it back. This employs the same group of muscles. If neither of these techniques works
for you, ask your doctor for help.
Many people also find it difficult to work the pelvic floor muscles without also tightening the abdominal and
buttock muscles, but stick with it. You'll get the knack eventually. Checking in a mirror or putting your hands
on your abdomen may help. Be sure to keep breathing normally, since holding your breath makes it harder for
the muscles to work properly.
Your doctor will help you decide how many Kegels you should start with and what a reasonable goal per day
should be. Here are some general tips:
• Start while lying down. This is easier for most people in the beginning; bending your knees or putting your legs up on a stool or

pillow will make it even easier. Eventually you'll be able to do the exercises while standing up or sitting.
• Breathe out as you contract and in as you release.
• Be patient. At first you may not be able to contract the muscles for more than a second or two, and you may feel overwhelmed at
the lack of control. It will improve if you keep trying.
• Go slowly. It's not a race. Tighten for a count of 5 and release slowly. (Eventually, you will probably hold for a count of 10.)
Repeat, building up to the number of repetitions you discussed with your doctor, usually 10 per session 3 times a day at the start,
building up to 100 or more. Take a brief rest between contractions.
• Find a way to build Kegels into your daily life. If you drive, do them at stop lights, for example, or work them in while cooking
meals or talking on the phone.
• Women can check on the exercise during sexual intercourse because, if it is done properly, the pelvic muscles will tighten around
the penis. Ask your partner for feedback.
• Use your skill in tightening the muscles to hold back urine when you lift, cough, or sneeze. Always tighten the muscles first.
Tighten when you feel a strong urge to urinate and need to wait.
For more help on learning to do Kegels, an organization called National Association for Continence (NAFC)
offers an $8 audio cassette tape and manual that coach you through the exercises and offers encouragement to
keep you on track. To order, call NAFC at 1-800-BLADDER.
For women, the most common operations are for stress incontinence. There are several types, all aimed at
lifting the urethra into a better position so it can close during coughing, sneezing, and other activities. Three
common procedures, named for the doctors who developed them, are:
• The Kelly procedure, which uses an incision made through the vagina. Also known as anterior vaginal repair surgery, this operation
has achieved a 62 percent success rate in recent studies. Possible complications include infection and an inability to urinate.
• The Marshall-Marchetti-Krantz procedure, in which the incision is made through the abdominal wall. The operation, also known as
retropubic suspension, scored a 78 percent cure rate in recent studies. Possible complications include infection, inability to urinate,
and new onset of urge incontinence.
• The Stamey procedure, which relies on small incisions in the abdomen, as well as an incision in the vagina. Also known by the
imposing name of needle bladder neck suspension surgery, this operation promises an 84 percent cure rate. Possible complications
include infection, inability to urinate, and new onset of urge incontinence.
Recently, a "no-incision" surgery technique has been developed which requires only two small punctures above
the pubic bone and no vaginal incision. Another new technique is laparascopic surgery for bladder suspension,
which uses local anesthesia and requires less than 24 hours in the hospital. Both of these procedures are
appealing alternatives, but their long-term success rates are not yet known.
Less commonly, women may have an inflatable artificial sphincter implantation or a periurethral injection. If
you have severe stress incontinence, and other procedures haven't worked, your doctor may also suggest a
urethral sling procedure, in which a strong material is placed around the urethra to help it into position and
support it. A recent study evaluating the effectiveness of this procedure confirmed an 89 percent cure rate.
However, it does pose the threat of such complications as infection, possible erosion of the sling, formation of
an abscess, failure of the vaginal wall to heal, or urinary retention.
Thanks to their high success rates, collagen injections are also becoming a more widely used treatment for
urinary incontinence. However, this type of therapy holds its greatest promise for women. In one recent study,
75 percent of the women who received collagen periurethral injections enjoyed an improvement or cure, while
only 52 percent of the men experienced comparable results.
Bladder Catheterization
In some situations, the best way to treat incontinence is to use a catheter to empty the bladder on a regular basis.
There are two methods of catheterization: indwelling, in which the catheter is left in place, and intermittent, in
which the catheter is inserted and removed each time it's necessary to void. Indwelling catheters are used for
overflow incontinence caused by obstruction that cannot be corrected surgically and for people who have
difficulty getting to the bathroom. Intermittent catheterization is used for overflow incontinence when
medication fails to help the problem. By periodically clearing the bladder, it reduces the chance of leakage at an
inappropriate time.
If you are looking for products to help with incontinence, there are several mail-
order companies that specialize in them. Some will send a sample of a product that
interests you, if you ask. A good guide to these products is available from an
organization called National Association for Continence (NAFC). This group
publishes a $10, 100-page resource guide describing hundreds of products for
managing incontinence, with manufacturers, distributors, and mail-order retailers.
Call NAFC at 1-800-BLADDER to order.
Companies that sell incontinence products by mail and offer catalogs include:
A-Z Medical Supply
P.O. Box 670332
Houston, TX 77267
713-838-8353
ARC Home Health Products
101 Browne Street
Oneonta, NY 13820
800-278-8595
Direct Medical Inc.
5422 Kiam Street
Houston, TX 77007
800-659-8037
HDIS
9385 Dielman Industrial Drive
Olivette, MO 63182
800-269-4663
Living with Incontinence
Although most incontinence problems can be eliminated or improved, there may still be situations which call
for special products to cope with leakage. Some people need them while waiting for treatment or following
prostate surgery. Others use them for "insurance" during travel, or when they have important business meetings
or social events. Even when improved with treatment, incontinence sometimes remains a worry.
Fortunately, much progress has been made in the design of products for incontinent adults, including absorbent
underproducts, external collection devices, and general aids. Talk with your doctor about the best choices for
your situation, and don't hesitate to experiment. Some people find they do better using more than one type of
product. A super-absorbent bulky pad may be fine at home, but for a long plane ride, an external collection
device may be a better choice. There are also less bulky pad-and-pants combinations. New improvements are
constantly coming on the market, so check for the latest designs in the types of products that interest you. The
best new products used properly make it easy to maintain a normal lifestyle while managing incontinence.
Absorbent Underproducts
Absorbent underproducts can fit into almost any kind of activity, from exercise to sleep. Special underwear
designed to hold pads, absorbent underpants, or a combination of pads and pants can be worn under regular
clothing. They come in different shapes and sizes, for men and women, and vary in absorbency to meet
different needs. You may need to try several to find the best fit and design for you. A bulkier choice is the adult
undergarment, which uses Velcro or adhesive closures to adjust for size. For men, a cup-like pouch device
called a drip collector will cope with small amounts of urine. The pouch is lined with absorbent material and the
outside is a moisture barrier. It is held in place by a belt or fastened to underwear, and is not noticeable under
regular clothing.
External Collection Devices
These products use a drainage tube and collection bag and work in the same way as a catheter, except that no
parts enter the body. They fit around the penis for men and are attached to the genital area for women. The
design for men usually resembles a condom and drains into a collection tube. A belt, leg bands, and adhesives
hold it in place. The women's device is similar, but more complicated to attach securely.
General Aids
For people concerned about protection while sleeping, protective bed pads or cloths are available. The pads
come in a variety of sizes and absorbencies, both disposable and reusable, and are relatively inexpensive.
For women, there are a number of simple devices that make it possible to urinate while standing, making
urinating outdoors, or in less-than-clean public restrooms, more comfortable.
Special skin care products are available to help clean and protect the skin and prevent odor. Non-irritating and
non-drying, these wipes, cleansers, moisturizers, moisture barrier creams, and powders are specially formulated
for use by incontinent people. Special sprays, liquids, and even pills are available to help eliminate odor.
Sex and Incontinence
Incontinence can have a major effect on sexuality. Fear of leakage, embarrassment, and simple, practical hassles
can make sexual intimacy a challenge. Too often, people with incontinence simply withdraw from sexuality,
cutting themselves off from intimacy rather than dealing with the problem.
But incontinence needn't put an end to sexual expression. These problems can be overcome. The key is learning
to talk about your feelings, listening to your partner's feelings, and doing some practical planning to deal with

the situation.
Embarrassment is the biggest hurdle for most people. How do you tell a new partner about the problem? How
does a caring spouse come to terms with the situation? Some people find that a therapist or support group helps
break the ice; ask your doctor for a referral. Experts say that people dealing with incontinence may need to
expand their definitions of sexual expression, and learn to ask openly for cooperation in choosing positions that
don't put pressure on the bladder.
Fear of urine leakage during sex is a common problem. Wearing pads during foreplay and using absorbent bed
pads may help, and your doctor may be able to recommend ways of minimizing leakage, depending on the
cause of incontinence. It may take some experimenting, but don't give up; even men with an indwelling catheter
can have intercourse, with the help of a cooperative partner.
Source: From the PDR® Family Guide Series
Copyright ©2004 Thomson Healthcare. All Rights Reserved. privacy policy | about | license & disclaimer