Raymond Wayne Whitted MD, MPH, L L C
Patient Information
Patient Name:____________________________________________ Home Phone:______________________________
Nombre del Paciente Telefóno del Hogar
Home Address:___________________________________________ Work Phone:______________________________
Direccion del Hogar Telefóno del Trabajo
City:_________________ State:________ Zip Code:________ Date of Birth______________________________
Ciudad Estado Codigo Postal Fecha de Nacimento
Occupation:______________________________________________ Social Security:______________________________
Ocupacion Numero de Seguro Social
Employer:_______________________________________________ Marital Status:______________________________
Empleo Estado Civil
Emergency Contact:_______________________________________ Phone Number:______________________________
Contacto de Emergencia Telefóno
Referred By:_____________________________________________ Driver’s License #:______________________________
Referido Por Numero de Licencia de conducir
Allergies/Alergias:________________________________________ E-mail address:______________________________
** IF YOUR VISIT IS FOR A WELL WOMAN EXAM, CHECK HERE:____ Si su visita es para un examen annual, marque aqui:____
INSURANCE INFORMATION
Name of Primary Insurance: _______________________________________________________________________________________
Nombre del Seguro
Address:____________________________________________ Phone Number:__________________________________________
Direccion Telefóno
Group Number:_______________________________________ Policy or I.D. Number:____________________________________
Numero de Grupo Numero de Poliza
Name of Subscriber:___________________________________ Date of Birth:____________ Relation to Patient: ______________
Nombre del Asegurado Fecha de Nacimeinto Relacion al Paciente
Subscriber’s Employer: ___________________________________________________________________________________________
Empleo del Asegurado
Name of Secondary Insurance: _____________________________________________________________________________________
Nombre del Seguro Secundario
Address:__________________________________________________ Phone Number:__________________________________
Direccion Telefóno
Group Number:____________________________________________ Policy or I.D. Number:____________________________
Numero de Grupo Numero de Poliza
Name of Subscriber:________________________________________ Date of Birth:______ Relation to Patient: ______
Nombre del Asegurado Fecha de Nacimeinto Relacion al Paciente
Subscriber’s Employer: ____________________________________________________________________________________________
Empleo del Asegurado
FEES AND INSURANCE INFORMATION
All fees are payable at the time services are rendered. We accept Visa, Master Card. Your medical insurance is a contract between you and your insurance
carrier and the terms of the contract vary according to the terms of your policy. Final payment for all charges is the patient's responsibility and should ib be
necessary for this account to be turned over to either an attorney or collection agency for collection, I understand that I will be liable for any charges incurred,
including attorney's fees and court costs.
Todos los honorarios por servicio deben ser pagados al recibir el servicio. Aceptamos Visa, Master Card. Su seguro medico es un contrato entre usted y
compania de seguro. Pagos por nuestros servicios dependen de los terminos de su poliza. El pago final de todos los cargos es su responsabilidad. Si es
necesario tomar accion legal para cobrar esda deuda, usted es responsable de los gastos legales.
We have elected not to carry Medical Malpractice insurance or otherwise demonstrate financial responsibility. However, we agree to satisfy any adverse
judgments up to the minimum amounts pursuant to S.458.320 (5)(g). Florida Law imposed penalties against non-insured physicians who fail to satisfy
adverse judgments arising from claims of medical malpractice. This notice is pursuant to Florida Law.
PHYSICIAN'S RELEASE AND ASSIGNMENT
Thereby authorize payment directly to Raymond Wayne Whitted MD, MPH, LLC. of all benefits applicable and otherwise payable to me from my insurance
carrier, HMO or other third party payor, for services rendered by Raymond Wayne Whitted, LLC. I understand that I am financially responsible to Raymond
Wayne Whitted MD, MPH, LLC for any and all charges that the carrier declines to pay. I hereby authorize the release of my medical records as deemed
necessary for payment of insurance benefits.
Por la presente autorizo el pago directamente a Raymond Wayne Whitted MD, MPH, LLC, todos los beneficios derivados del seguro que ampara al paciente
y que normalmente yo tendria derecho de percibir. Con mi firma autorizo transferir documentos relacionados a mi tratamiento medico a mi compania de
seguro para processar mi reclamacion. Yo entiendo que soy responsable por todos los cargos no cubiertos bajo mi seguro medico.
1. I, the undersigned patient or _______________ (name of authorized representative acting on behalf of patient) consent to undergo all necessary
tests, medication, treatments, and other procedures in the course of the study, diagnosis, and treatment of my illness (es) by the medical staff and
other agents and /or employees of Raymond Wayne Whitted MD, MPH, LLC. The identity of the physician who currently has primary
responsibility for my care has been provided to me.
2. I understand that, absent emergency or extraordinary circumstances, non-routine and major medical procedures will not be performed upon me
until I have had an opportunity to discuss and agree to them with a physician.
3. I am aware that the practice of medicine and surgery is not an exact science and I acknowledge that no guarantees have been made to me as to the
results of diagnosis, examinations or treatments in the hospitals or offices.
4. I hereby authorize the staff of Raymond Wayne Whitted MD, MPH, LLC to take such still photographs, motion pictures, television transmissions,
and/or videotaped recording for educational and evidentiary purposes as they may wish.
5. I hereby grant access to medical records for bona fide research to members of the medical staff and other medical researchers and authorize my
medical records and results to be used for research. I realize that my records will not be identified as pertaining to me specifically without my
expressed permission.
6. I consent to the release of medical information to other institutions, agencies, health care organizations, or health care providers accepting the
patient for medical or institutional care, and consent to the release of medical information to the patient’s insurer and/or managed care
organization and their agents for purposes including but not limited to Utilization Review and Quality Assurance Review.
7. I hereby authorize payment directly to Raymond Wayne Whitted MD, MPH, LLC of benefits due to me in my pending claim and/or MAJOR
MEDICAL BENEFITS otherwise payable to me, but not to exceed the Hospital and/or Physician’s regular charges for this period of treatment. I
agree that a photostatic copy of this authorization is as valid as the original.
I have read and clearly understand the above.
_____________________________________ Date:______________ Time:_______________ AM/PM
Signature of patient or patient’s authorized representative
_____________________________________
Witness’ Signature
MINOR’S CONSENT: Un-emancipated patients (minors under 18 years of age) must have parents or guardians signature, except for emergency
medical care, diagnosis or treatment of a sexually transmitted disease, or treatment of pregnancy.
_____________________________________
Parent or Guardian’s Signature
EMERGENCY CONSENT: Patient is unattended by legal guardian, health care surrogate, or relative and/or unable to sign consent for treatment
necessary to correct or stabilize a serious medical condition (s) demanding immediate medical attention. I certify that this condition will endanger the
life, limb or health of the patient and authorize emergency procedures
______________________________________ Date: ________________ Time: _______________ AM/PM
Physician’s Signature
Raymond Wayne Whitted MD, MPH
…dedicated to healthy lifestyles and safe, state-of-the-art, innovative surgery for women of all ages
...because quality is an experience!
EDUCATORS
Community Programs
CME Programs
Surgical Preceptor
R. Wayne Whitted MD, MPH
Diplomate, ABOG
Certified in Advanced Laparoscopy
Certified in Advanced Hysteroscopy
Certified Menopause Clinician
Certified Bone Densitometrist
Certified Researcher
Certified Wartime Surgery
COMPREHENSIVE
GYNECOLOGY &
MINIMALLY
INVASIVE SURGERY
Abnormal Pap Smears
Advanced Colposcopy
Abnormal Periods
Bladder Prolapse
Chronic Pelvic Pain
Endometriosis
Ectopic Pregnancy
Family Planning
Fibroids
Genital Warts
Immunizations
Loss Of Urine
Menopause
● Risk Assessment
● Support Series
Ovarian Cysts
Rectocele
Surgical Gynecology
Hysteroscopy
Laparoscopy
Vaginal Surgery
Surgical Support Series
Uterine Prolapse
Vaginal Prolapse
Vaginal Infections
Vulvodynia/Vestibulitis
Well-Woman
COMPREHENSIVE
RESEARCH
Laparoscopy
Hysteroscopy
Menopause
Women’s Health
8740 N. Kendall Drive, Suite 101, Miami, Florida 33176
Phone 305 596 3744 ● fax 305 596 3676● www.drwhitted.net
MEMBERSHIPS
Obstetrics and Gynecology
Gynecologic Laparoscopy
Bone Densitometry
Colposcopy and abnormal paps
Physician Executives
Honor Medical Society
Best Doctors
AESTHETIC GYNECOLOGY
Botox
Vaginal Rejuvenation
Permanent Hair Removal
OFFICE PROCEDURES
Hysteroscopy
LEEP cone biopsy
Cryosurgery
Dilation and Curettage
Ultrasound
Urodynamics/Bladder Studies
Heel Density Scan
www.drwhitted.net
Notice of Privacy Acknowledgement
Notificacion De Privacidad En Las Practicas Medicas
I have read and understood the Notice of Privacy Practices.
(Yo he leido y comprendo la Notificacion de Privacidad en las Practicas Medicas)
Date (Fecha)________________________________________________________________________
Patient’s Name Printed ( Nombre de Patiente ) ___________________________________________
Patient’s Signature (Firma de Patiente)__________________________________________________
Witness ____________________________________________________________________________

1
www.drwhitted.net
R. Wayne Whitted MD, MPH
8740 N Kendall Dr. Suite 101
Miami, Florida 33176
Phone: 305-596-3744
As part of our commitment to women’s healthcare we now offer a variety of Aesthetic/Cosmetic enhancement
procedures using the McCue Energist Ultra Variable Pulsed Light system (VPL). The VPL is one of the most recent
advancements for virtually PAINLESS permanent hair removal. In addition, with this we can treat a variety of other
skin abnormalities: SUN-DAMAGED SKIN, THREAD VEINS, STRETCH MARKS, ANGIOMAS AND MORE.
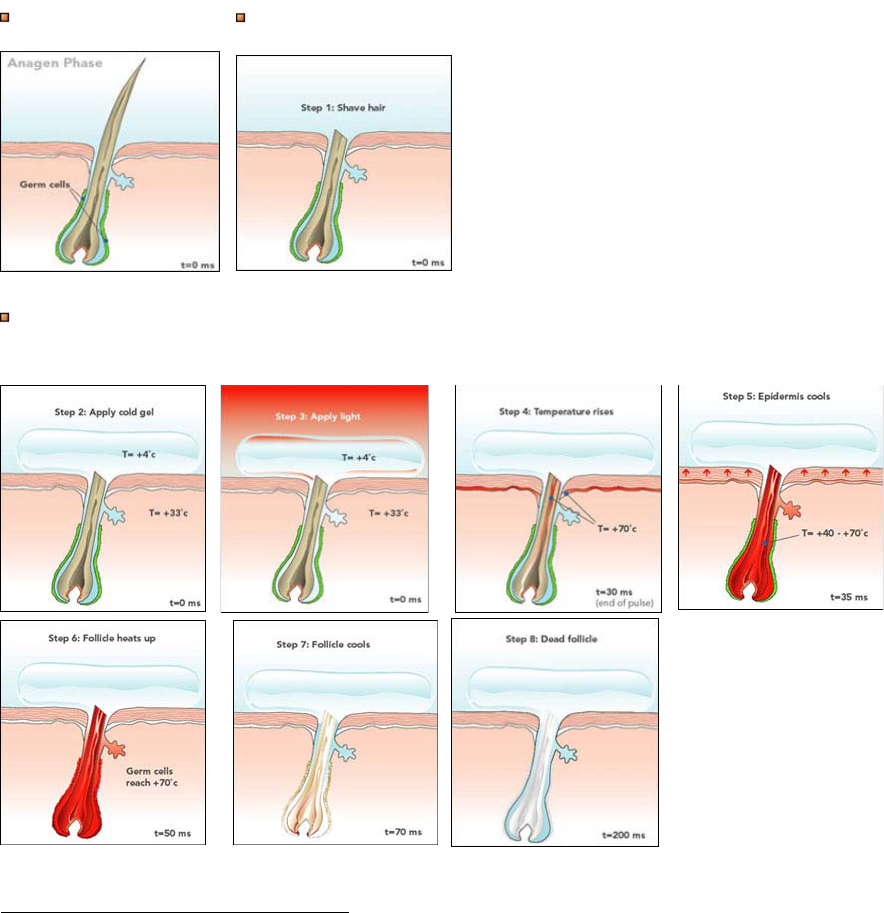
Goal - Destroy the hair follicle and achieve 'hair free'. Laser and Pulsed Light are both Light based ways to do hair reduction. These
Light based treatments only work on hair that is in the active growing, or Anagen, phase. At any given time, only about 25% of the hair
on our body is in the appropriate stage (phase) for treatment. The other 75% cannot be affected by light treatments. That is why it is
necessary to perform multiple treatments with Laser and with Pulsed Light.
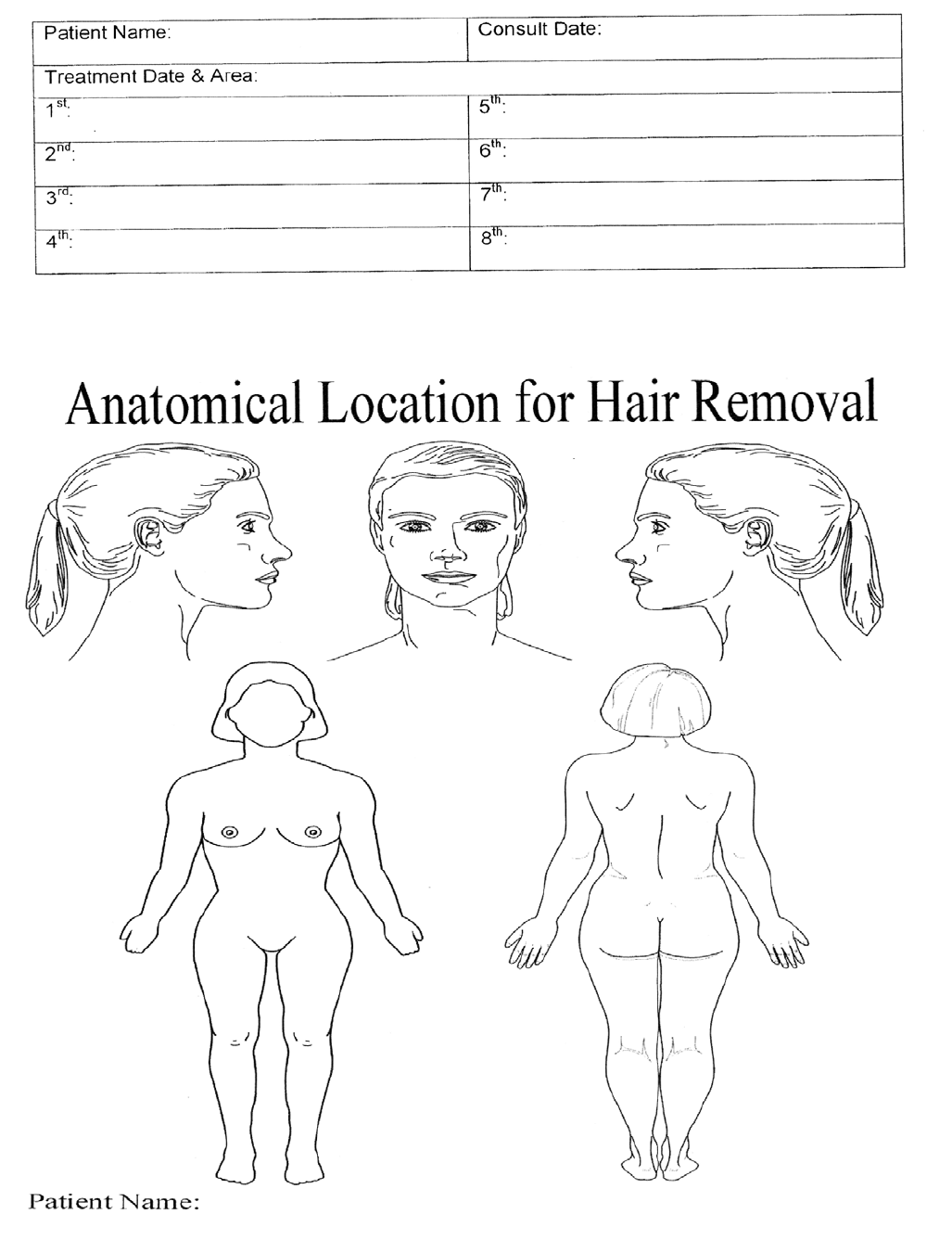
HAIR REMOVAL
How - Traditional Laser and Intense Pulsed Light systems convert light energy into heat. The Melanin in hair absorbs more of the heat
than the surrounding skin tissue. The heat transfers down the hair shaft, and if the temperature at the base of the hair shaft reaches
70° C, the follicle will be destroyed - no more hair!
VPL™ takes this process a step further. By changing the number of pulses in each 'shot', the length of the individual pulses, and most
importantly the space, or Delay, between each pulse, the ULTRA can more specifically target different color hairs on different skin
types.
The ULTRA VPL™ is the most versatile (and effective) hair removal system that you can buy!
Raymond Wayne Whitted MD, MPH, FACOG
…dedicated to safe, state-of-the-art surgery and health life-styles for women of all ages
…because you deserve the best!
2
Treatments
Active growth stage.
Shave the area to be treated.
Apply a thin layer of gel to the area. This gel acts as a 'coupler' which intensifies the light, and makes a great guide for the area to be
treated.
SKIN TREATMENTS USING VPL SYSTEMS
The concept of using Intense Pulse Light sources for the treatment of many skin conditions associated with the aging process is
currently receiving considerable interest within the professional beauty industry and the general public. There exists today a rapidly
growing demand for addressing the signs of aging with safe simple techniques. Until the recent introduction of Intense Pulsed Light
(IPLT) and more recently Variable Pulsed Light (VPL™) treatment (initially, successfully developed for hair depilation), the only available
treatments included surgery, chemical peeling, ablative and non-ablative resurfacing, microdermabrasion and various visible light and
near IR laser treatments.
VPL skin treatment is a process that has many advantages over other treatment modalities as it effectively treats a combination of
changes in the skin, from the signs of ageing, over exposure to the sun, broken facial capillaries, pigmentary abnormalities and
cosmetic imperfections.
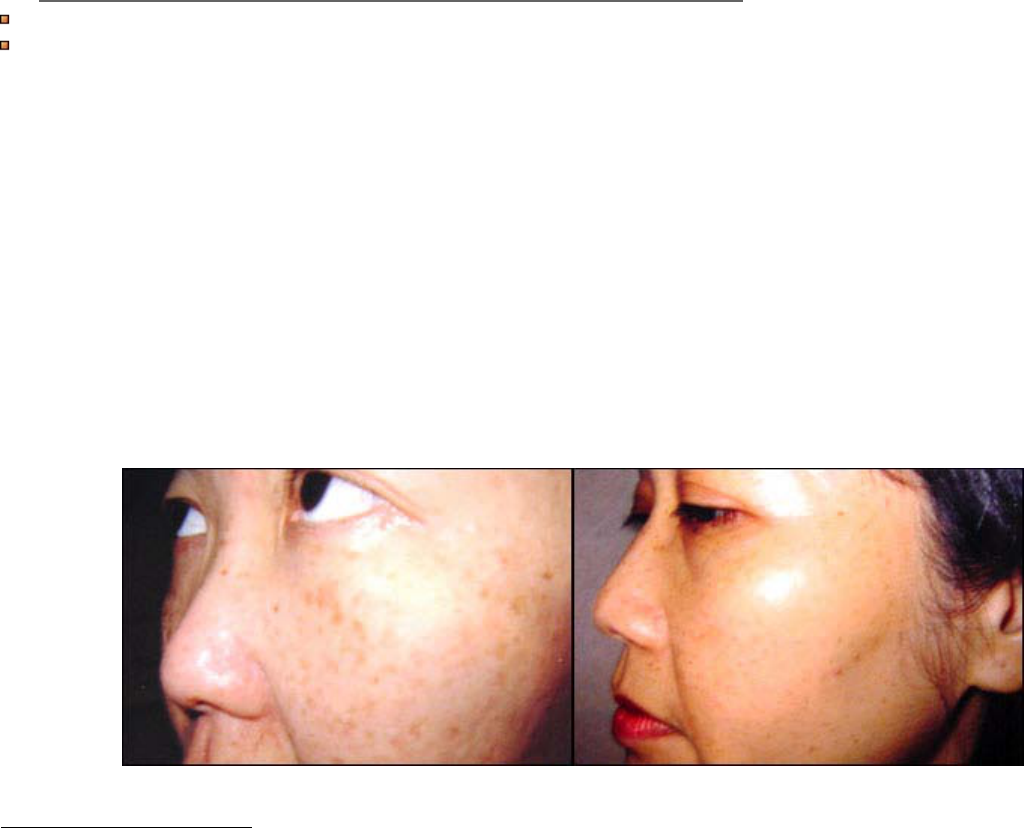
Sun Damaged Skin
Sun damaged skin occurs as the result of excessive exposure to ultraviolet (UV) light, which induces epidermal and dermal changes.
Skin affected in this way is characterised by thinning of the epidermis and dermis, coarse skin texture, wrinkling, Telangiectasias and
changes in pigmentation.
The overall appearance of sun-damaged skin relates to the resultant UV damage of structural components such as collagen and elastin
fibres. Appearance is also affected by genetic factors, intrinsic factors, disease process such as Rosacea, and the overall loss of
3
cutaneous elasticity associated with age. More people now have extended periods of sun exposure and, coupled with the thinning of
the ozone layer and other factors, this has resulted in visible signs of ageing, damage and disease evident in ever-younger people.
People in their twenties and thirties are now witnessing solar elastosis, Telangiectasia, solar lentigines and rhytide formation.
Treatment Process
The McCue ULTRA VPL™ System is suitable for full face, neck, chest and hands treatment to improve the visible signs of sun damage
and ageing.
The treatment of sun-damaged skin includes treating both benign pigmented and vascular lesions. Exposure to UV light destroys skin
cells thereby slowing down the growth of new skin and the production of collagen. The increase in blood flow as a result of the
treatment to the region will also bring fresh supplies of oxygen and nutrients to the cells, which will assist in the removal of waste. By
traumatizing the epidermis and dermis the skin will also be encouraged to go into 'repair mode' increasing cell turnover
***Other treatments using the McCue ULTRA VPL™ include the following:
The treatment of benign pigmented epidermal and cutaneous lesions including warts, scars, chloasma, and striae.
The treatment of benign cutaneous vascular lesions including port wine stains, Hemangiomas, facial, truncal and leg
telangiectasias, Rosacea, melasma, angiomas and spider angiomas, poikiloderma of Civatte, leg veins, facial veins and
venous malformations
Benign Pigmentation Treatment
Benign pigmented conditions are caused by the melanocytes having an irregular production of melanin. The treatment involves the
'disabling' of rogue melanocytes by directing energy of the correct fluency and wavelength to these over-producing melanocytes, which
automatically absorb more energy than normal melanocytes because of their darker color. Following treatment the production of
melanin will become normal and the skin will return to its ambient color. Energy fluency settings sufficient to cause erythema in the
ambient skin areas are usually sufficient to disable those melanocytes in the darker skin pigmentation.
Number of treatment sessions required
Generally, between four to six treatment sessions are required, although it depends upon the treatment type and the area being
treated. A good 'rule-of-thumb' is to assume one treatment for each decade of a person's life. The number of treatment sessions may
increase when treating darker skin types. Normally, these treatment sessions are carried out at three week intervals.
3 Treatments at 3 week intervals
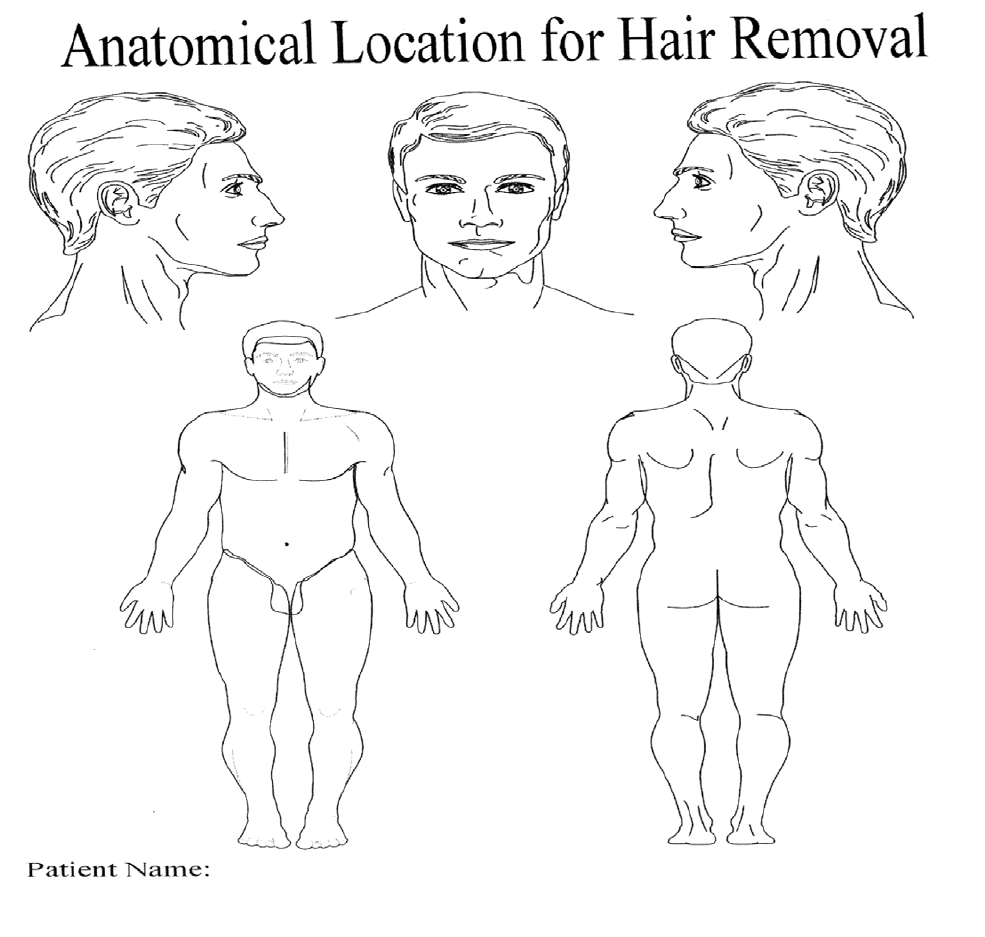
Areas to be Treated
Abdomen Armpits Back Bikini Buttocks Cheeks Chest
Chin Ears Eyebrows Feet Fingers Forearms Full Arms
Full Legs Hands Lower Legs Neck Shoulders Thighs Upper Arms
Upper Lip Other _____________________________
4
What are your realistic goals?
What concerns do you have regarding treatment?
Do you have any questions regarding the treatment procedure?
Number of treatment sessions required
Hair Removal
Generally, between three to six treatment sessions are required, although it depends upon the area being
treated. The aim of each treatment is to reduce the hair density successively to a level that is satisfactory to the
client.
The number of treatment sessions may increase when treating darker skin or lighter hairs since the percentage of
hair removed during each treatment will be reduced in these instances.
Period between successive treatments
Due to the cyclical nature of hair growth, a number of treatments are required in order to ensure that treatment
covers the growth stage of all follicles. It is only during the growth stage, with the hair present, that the
follicles can be successfully treated.
It is recommended that each treatment be performed once when the next phase of hair has grown through, this
time period varies depending on the area of the body and on the individual. For example, the hair on the upper lip
has a growth cycle of approximately 6 weeks, whereas the growth cycle for leg hair is about 24 weeks, so it may
not be necessary for a Client to return for a second treatment on their legs until about 8 weeks later. Since growth
cycles can vary significantly between individuals, a good indication of the period between successive treatments
can be obtained from the Clients themselves. When the Client considers that they have a full re-growth of hair then
it is most probably time for the next treatment.
Note: At the start of each subsequent treatment the same safety steps that are recommended for the
first treatment should be completed. To ensure that subsequent treatments produce favourable
results,
the Client must inform the Operator if any pigmentary changes have occurred.
If so
then these should be assessed individually, but generally an increase in the amount of melanin in the
skin would indicate that a lower energy should be used.
What to Expect After Treatment
The immediate after effect is that the treated area should become slightly red, particularly around the hair.
Typically, this redness will disappear in a matter of a few hours at most (and often in just a few minutes) with the
skin then returning to its normal color. The hair will still be in place in the follicle since the treatment, unlike laser,
is not a vaporizing process.
During the next ten days or so the hair will appear to continue growing, albeit more slowly than before. What
actually is happening is that the hair is no longer supported by the follicle but is being pushed out by the growth of
the epidermix which is still in close contact with the hair shaft. If left alone, the treated hairs will fall out naturally
after a period of between one and three weeks, dependent on the depth of the hair root. The hair is acting as an
effective barrier to infectioin of the inflamed follicle, and so they should not be removed prematurely.
After Care
5
Immediately following the treatment session, or at regular intervals in the case of treatment of large areas,
soothing gel should be applied to the treated area. Recommended gels include Witch Hazel, Tea Tree or Aloe Vera.
These gels have the effect of cooling the area and generally include antiseptic properties to protect the damaged
follicle against opportunistic infections.
The Client should be advised to refrain from using cosmetic make-up, perfumed soaps and similar products for
about 24 hours following treatment. Also, exposure to the sun should be avoided for about one month unless a
high factor sun block is used as a precaution against exacerbating any pigmentary changes which may not be
immediately evident.
Health History Form
Patient Number:
Address
Patient Name
Date of birth
Sex: Female Male
Doctor’s Name:
Operator’s Name:
Date:
It is not recommended that treatment be carried out on Clients
suffering from the following (CONTRAINDICATIONS)
Pregnancy
Epilepsy (flashes of light may cause seizures)
History of light sensitive rashes
Recent suntan (within 1 week)
Undertaking treatment involving blood thinning medication (possible bleeding)
History of Keloids
Oral acne medication in the last six months (Accutane)
Photosensitivity in the last six months
Medication for which sunlight is contraindicated (see information on drug induced
photosensitivity)
Kaposi’s sarcoma
Malignant or suspicious tissues
History of poor wound healing
Tattoo over treatment area
Conditions that require a medical consultation prior to treatment:
Hairy Moles (can be precancerous)
Diabetes (issues with tissue healing)
Contraindicated Medications
Malignant or suspicious lesions (a sight of therapy)
Hemophilia
Photosensitivity
Please answer the following questions: Please circle the appropriate answer
Skin type
Oily Sensitive Dry Other
Skin Color
White Olive Oriental Indian Afro-Caribbean

6
Moles Freckles Acne Psoriasis Eczema
Skin Conditions
Shingles Herpes Keloid Pigmented patches Vitiligo
What other cosmetic procedures have you undertaken? Please Circle
Face Lift Laser Resurfacing Hair Removal Botox Cosmeceuticals Chemical Peels
Pulsed Light Dermabrasion Other: ________________________________________
How would you describe your reaction to the sun? Please Circle
Type 1 (1): Always burn, never tan
Type 2 (2): Sometimes burn, then tans
Type 3 (3): Always tan, rarely burns
Type 4 (4): Rarely burns, tans with ease
Type 5 (5): Moderately pigmented, tans profusely
Type 6 (6): Deeply pigmented, never burns
Are you taking medications that may make your skin photosensitive?
Yes No ________________________________________________________
________________________________________________________
Photosensitivity
There are many forms of medication and products available that can cause the skin to become sensitive to
light. These drugs can be taken by mouth or applied to the skin, therefore it is important to ascertain
whether the client is currently using these products or undergoing a course of medication.
When receiving a light based treatment, a reaction can sometimes occur, with varying degrees of severity.
This varies greatly from client to client and ranges from no noticeable reaction through to blisters and
severe skin responses. This reaction is called “Drug-Induced Photosensitivity” and can be divided into two
groups:
Photo-toxic Reactions: these are dose related and can be seen to slight degree in people who are
exposed to sunlight.
Photo-allergic Reactions: these involve the immune system and may be similar to other allergic
reactions such as swelling, rashes and hives.
It is due to these reactions that it is advisable to ensure test patches are
performed to determine if any adverse reaction occurs.
Common Drugs that can cause photosensitive reactions:
Use of these drugs does not exclude a patient from treatment but a test patch should
Be performed and patient should sign a release:
Xanax, Elavil, Benzocaine, captopril, Librium, Chloroquine, Tetraccline, Ciprofloxacin, Bactrim, Dapsone,
Diltiazem, Benadryl, Penetrex, 5-FU, Glyburide, Griseofulvin, Haldol, Hydralazine, Advil (Motrin), Isoniazid,
Accutane, Methotrexate, Rogaine, Naprosyn (aleve), Nifedipine, Norfloxacin, Nortriptyline, Birth Control
Pills (estrogen of any kind), Floxin, terramycin, Perfenazine, Phenylbutazone, Dilantin, Feldene, Compazine,
7
Phenergan, Vivactil, Quinidine, Quinine, Sulfur antibiotics, Mellaril, Navane, Tolinase, Retin-A, Stellazine,
Vitamin A
Initials _________
COMMON DRUGS THAT CAN CAUSE PHOTOSENSITIVE REACTIONS
*indicates high incidence of drug induced photoreactions
Antibiotics
Doxycycline,
Demeclocycline, Tetracycline, Vibramycin
Declomycin
Nalidixic Acid
Fluoroquinolones
Blood Pressure & Heart Medications
Hydrochlorothiazide
Furosemide
*
Amiodarone
Drugs
Phenothiazines
PABA and or PABA esters
Herbals:
St. Johns Wort
Melaton in
Kava Kava
Initials _________
Do You Have any Allergies? Yes No
Do You have personal history of skin cancer? Yes No
Do You have any medical condition or serious illness? Yes No
If yes, ____________________________________________________________________
8
Treatment Checklist (Complete before each treatment)
1. Does the patient have any of the contra-indications? Yes No
2. If the patient has a sun tan, was it within the last 4 weeks? Yes No
3. Does the patient have any skin abnormalities which may be of concern? Yes No
4. If the patient has received previous treatments, have they had any problems? Yes No
CONSENT FORM
NAME _______________________________ DOB __________ DOS __________
PHONE ________________ ADDRESS ___________________________________
I understand that the procedures is an elective cosmetic procedure and hereby
acknowledge the following:
_____1. I understand that the extent of the effectiveness of the treatment using
intense pulsed light varies from person to person and therefore the response to
treatment can also vary.
_____2. I would like the following area of my body to be treated: _____________
I understand that immediately following treatment (post) the area may appear
reddened and there is a slight chance that small blisters may appear.
_____3. I understand also that following the first treatment I may not see an
immediate effect and will need to have a second/third/fourth/future treatment.
_____4. I understand that, following treatment, there is a slight possibility, that
depigmentations of the area being treated may occur causing the skin to appear
darker. These symptoms, should they occur, are usually temporary and slight but
there is no absolute guarantee that all normal pigments returns. I understand that
there is a very slight risk of scarring with any skin treatment but in this case it is
extremely small.
_____5. I confirm that I have provided the office/Operator with any medical
details, which may be relevant to my treatment.
_____6. Photos are used to follow treatment and will be kept confidential and in
your personal record.
My signature below constitutes my acknowledgement that I have read, understand
and fully agree to the proposed treatment and that the process has been
satisfactorily explaned to me and I have all the information which I require.

9
Patient Signature ______________________________ Date ______________
Witness ______________________________________ Date ______________
Pre and Post Treatment Instructions
1. The Area being treated cannot be exposed to the sun. A broad spectrum
(UVA/UB) sunscreen SPF 30 or greater should be applied whenever exposed
to the sun. A sunscreen is available for purchase in our office if you do not
have one.
PULSED LIGHT HAIR REDUCTION
2. Do not tweeze, wax, or use a depilatory agent for one month prior to
treatment.
3. The area should be shaved 24-36 hours prior to treatment. A small stubble
must be visible.
4. Makeup, deodorant, perfumes or powder must be removed on the areas to be
treated.
5. Your treatment cannot be performed if you have a suntan or sunburn.
6. Immediately following treatment, the area may show slight to moderate
redness with some swelling. Blistering my occur.
7. During the healing phase, the area must be treated delicately. Do not rub,
scratch, or pick. If a crust develops let it fall off on its own.
8. Apply a thin layer of post laser lotion to the treated area several times a day to
keep the area moist.
9. Do not scrub the area. Pat the area dry. Do no shave over the area if swelling,
crusting, or scabbing is present.
10. If swelling occurs, you may apply ice wrapped in a soft cloth. Any discomfort
or stinging can be relieved with Tylenol.
11. If makeup is allowed, it must be applied and removed delicately. Excess
rubbing can open the treated area, increasing the chance of scarring.
12. Avoid excess perspiration for 48-72 hours after treatment.
13. In case of signs of infection (pus, tenderness, fever), contact the office
immediately.
14. The treated hairs will exfoliate or push out in approximately two weeks.
10
They do not fall out immediately.
Patient Signature ________________________________ Date _____________
Witness _______________________________________ Date ______________
POST-TREATMENT CARE INSTRUCTIONS
Skin Treatments
1. The area treated may be red and warm for a few hours following treatment. If
this is uncomfortable the patient should cool the area with a cold
flannel/towel or some other means of cooling. Do not use an icepack as this
may cause an “ice burn”.
2. Soothing preparations may be used providing they do not contain anti-
inflammatory or blood thinning properties. The patient should avoid
preparations such as Aloe Vera, Tea Tree Oil, Ibuleve, Difflam, etc.
3. If possible, the patient should avoid taking anti-inflammatory or blood
thinning medication for at least 7 days. Products include ibuprofen, aspirin,
etc.
4. The patient is advised not to smoke or drink alcohol for at least two hours
before and after treatment.
5. If the patient can refrain from the use of make-up that day this will also help
the skin to cool naturally.
6. For 2 days following treatment, the patient should only use cleansing products
that have been developed for sensitive skin. Be gentle when drying or rubbing
the area treated.
7. The patient should avoid tanning beds or sunbathing for at least 7 days after
the treatment.
8. If the patient is unsure about any after effects following treatment they
should contact the clinic for further advice.
Patient Signature _____________________________ Date ________________
Witness ____________________________________ Date _________________
11
12
13