About Vulvodynia
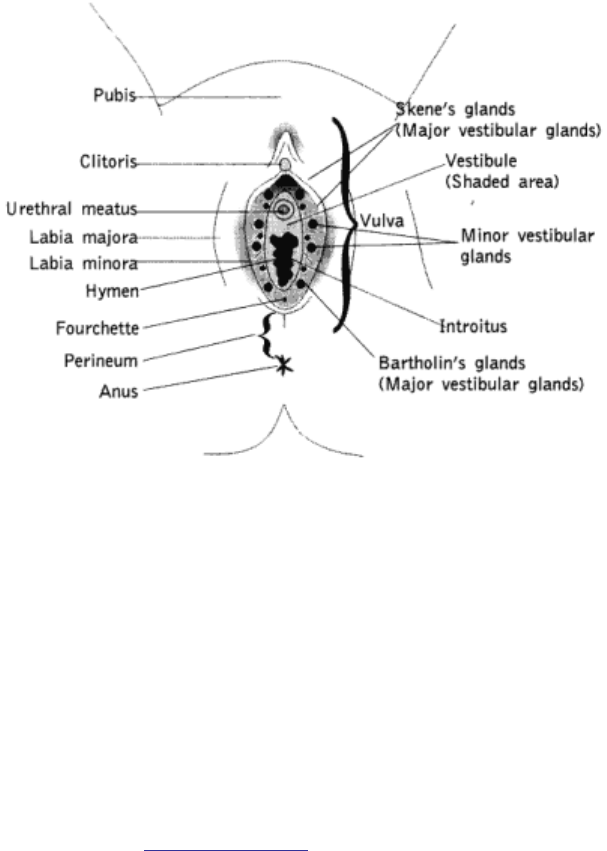
The vulva is the external part of the female genitalia. The outer and inner lips of the vulva are called the labia majora and
labia minora. The vestibule surrounds the opening of the vagina and the urethra. The openings to the Skene’s and
Bartholin’s glands are located within the vestibule. The perineum is the area between the bottom of the vulva and the anus.
Vulvar Anatomy
About Vulvodynia
The International Society for the Study of Vulvovaginal Disease (ISSVD) defines Vulvodynia as chronic vulvar discomfort or
pain, characterized by burning, stinging, irritation or rawness of the female genitalia in cases in which there is no infection or
skin disease of the vulva or vagina causing these symptoms. Burning sensations are the most common, but the type and
severity of symptoms are highly individualized. Pain may be constant or intermittent, localized or diffuse.
What is Vulvodynia?
Vulvodynia has been classified into the following subtypes:
Generalized (or dysesthetic) Vulvodynia
Dysesthetic Vulvodynia symptoms may be diffuse or in different areas at different times. Pain may be present in the labia
majora, labia minora, and/or the vestibule. (
see vulvar anatomy) Some women experience pain in the clitoris, mons pubis,
perineum and/or the inner thighs. The pain may be constant or intermittent. Symptoms are not necessarily caused by touch
or pressure to the vulva, i.e., with intercourse or bicycle riding, but these activities often exacerbate the symptoms.
Vulvar Vestibulitis Syndrome
Women with VVS have pain only in the vestibule, and only during or after touch or pressure is applied. Burning sensations
are the most common symptom and may be experienced with some or all of the following: sexual intercourse, tampon
insertion, gynecologic examination, bicycle riding, and wearing tight pants.
There are several other conditions that cause chronic vulvar pain and may coexist with Vulvodynia. The most common of
these are listed below:
Cyclic Vulvovaginitis
Women with cyclic vulvovaginitis have recurrent burning and itching symptoms at the same stage of the menstrual cycle.
Many have cyclical bouts of yeast infections and some have other causes for their symptoms.
Vulvar Dermatoses
There are many dermatologic conditions that may cause pain in the vulva. The most common include: allergic or contact
dermatitis, lichen sclerosus, lichen simplex chronicus and lichen planus. These conditions may cause symptoms of itching
and burning. Scratching the vulva and overusing topical medications may inflame the tissue, causing swelling and additional
pain.
Vulvodynia, as with most chronic pain conditions, can have a profound impact on a woman’s quality of life. It typically affects
her ability to engage in sexual activity and may interfere with daily functioning, e.g., sitting at a desk, engaging in physical
exercise, and participating in social activities. These limitations can negatively affect self-image and lead to depression.
The causes of Vulvodynia are still unknown, largely due to lack of research on the disorder in past years. Current research
studies are investigating possible causes of Vulvodynia and delineating risk factors for developing Vulvodynia. The medical
community speculates that potential causes of the condition may be:
What Causes Vulvodynia?
• an injury to, or irritation of, the nerves that innervate the vulva
• an abnormal response of different cells in the vulva to environmental factors (such as infection or trauma)
• genetic factors associated with susceptibility to chronic vestibular inflammation
• a localized hypersensitivity to candida (yeast)
• spasms of the muscles that support the pelvic organs
There is no evidence that Vulvodynia is caused by an active infection and it is not a sexually transmitted disease.
About Vulvodynia
To diagnose Vulvodynia, medical specialists will carefully review your medical history. You will be asked questions about
your symptoms, sexual activity, diet, feminine hygiene, previous medical problems and medication use. Your doctor should
also carefully examine the vulva, vagina and any vaginal secretions for other causes of your pain such as infections and skin
disorders. Many doctors will perform routine fungal vaginal cultures to ensure that an infection is not causing or worsening
any irritation or burning. A "q-tip test" may be administered during your exam. During this test, different areas of the vulva
and vestibule are touched with a Q-tip to determine the location and severity of your pain. If your doctor sees areas of skin
that look suspicious during your exam, a biopsy of the skin may be required. Additionally, he/she may look more closely
through a magnifying glass at any abnormal lesions in the vulva or may recommend a colposcopy, a test in which an
instrument is used to look at the vulva more closely.
Diagnosis
About Vulvodynia
Treatment
There is currently no "cure" for Vulvodynia. Treatments are directed toward alleviation of symptoms and may provide partial
or complete relief. It is important to keep in mind that the cause of vulvodynia is unknown and each woman’s symptoms are
unique; no single treatment works all the time or is appropriate for every patient. Some women respond very well to a
particular treatment, while others respond poorly or experience unacceptable side effects. It takes time to find a treatment or
combination of treatments that will decrease or alleviate your pain.
Some of the current treatments available (not listed in order of efficacy) include:
• Discontinuation of all topical medications, soaps, douches, etc., that can worsen irritation
• Local anesthetics (i.e. lidocaine)
• Tricyclic antidepressant medications (e.g., amitriptyline, nortriptyline, desipramine) See Fall 1999, Summer 2001,
Spring 2002 issues to read more
• Anticonvulsants (e.g., Tegretol, Neurontin) See Fall 1999, Summer 2001, Spring 2002 issues to read more
• Interferon injections Read More
• Nerve blockades, Read More
• Topical estrogen cream
• Pelvic floor therapy (for patients who have pelvic floor muscle abnormalities as measured by surface
electromyography)
Read More
• Physical therapy See Summer 1996 and Winter 2002 to read more
• Diet modification Read More
• Surgery (for vulvar vestibulitis syndrome only) Read More