F REQUENTLY A SKED Q UESTIONS
womenshealth.gov
1-800-994-9662
TDD: 1-888-220-5446
●
Radical. Removes the uterus, the
cervix, the upper part of the vagina,
Hysterectomy
and supporting tissues. (This is done
in some cases of cancer.)
Q: What is a hysterectomy?
Often one or both ovaries and fallopian
A:
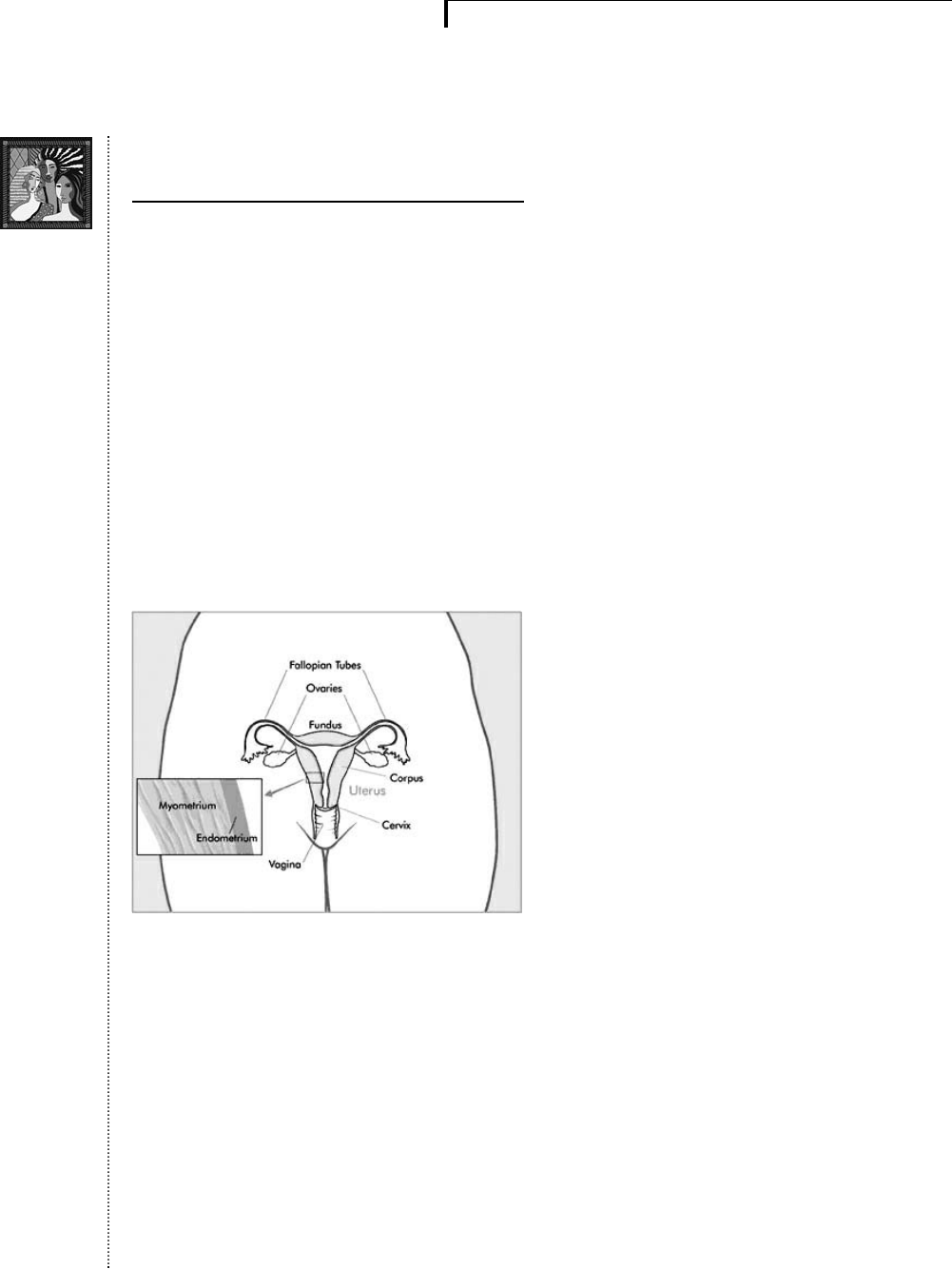
A hysterectomy is an operation to
tubes are removed at the same time a
hysterectomy is done.
remove a woman’s uterus (womb). The
uterus is where a baby grows when a
woman is pregnant. In some cases, the
ovaries and fallopian tubes also are
If you haven’t reached menopause
(when you haven’t had a period for 12
months in a row), a hysterectomy will
removed. These organs are located in a
stop your monthly bleeding (periods).
woman’s lower abdomen (see image
You also won’t be able to get pregnant.
below). The cervix is the lower end of
the uterus. The ovaries are organs that
produce eggs and hormones. The fal-
And you may have menopausal symp-
toms, such as hot f lashes and vaginal
dryness. If both ovaries are removed as
lopian tubes carry eggs from the ovaries
well, you will suddenly enter
menopause.
to the uterus.
Q: How common are hysterec-
tomies?
A:
A hysterectomy is the second most
common surgery among women in the
United States. (The most common is
cesarean section delivery.) Each year,
more than 600,000 are done. One in
three women in the United States has
had a hysterectomy by age 60.
Q: How is a hysterectomy
performed?
NATIONAL CANCER INSTITUTE
A: Hysterectomies are done through a cut
in the abdomen (abdominal hysterecto-
There are several types of hysterec-
my) or the vagina (vaginal hysterecto-
tomies:
my). Sometimes an instrument called a
●
Complete or total. Removes the
cervix as well as the uterus. (This is
the most common type of hysterec
-
tomy.)
laparoscope is used to help see inside
the abdomen during vaginal hysterecto
-
my. The type of surgery that is done
depends on the reason for the surgery.
●
Partial or subtotal. Removes the
Abdominal hysterectomies are more
upper part of the uterus and leaves
common and usually require a longer
the cervix in place.
recovery time.
page 1
N A TIONAL W OMEN’ S H EAL TH I NFORMATION C ENTER
U.S. Department of Health and Human Services, Office on Women’s Health
womenshealth.gov
1-800-994-9662
TDD: 1-888-220-5446
page 2
F REQUENTLY A SKED Q UESTIONS
Q: How long does it take to recover
●
Uterine prolapse. This is when the
from a hysterectomy?
uterus moves from its usual place
A:
Recovering from a hysterectomy takes
time. You will stay in the hospital from
one to two days for postsurgery care.
Some women may stay in the hospital
up to four days.
down into the vagina. This can lead
to urinary problems, pelvic pressure,
or difficulty with bowel movements.
●
Cancer. If you have cancer of the
uterus, cervix, or ovary a hysterec
-
●
Abdominal. Complete recovery
usually takes four to eight weeks.
You will gradually be able to
increase your activities.
tomy may be part of the treatment
your doctor recommends.
●
Persistent vaginal bleeding. If
your periods are heavy, not regular,
●
Vaginal or laparoscopic. Most
women are able to return to normal
activity in one to two weeks.
or last for many days each cycle and
nonsurgical methods have not
helped to control bleeding, a hys
-
terectomy may bring relief.
For both, by the sixth week, you
should be able to take tub baths and
●
Chronic pelvic pain. Surgery is a
resume sexual activities.
last resort for women who have
chronic pelvic pain that clearly
comes from the uterus. However,
Q: Why do women have hysterec-
many forms of pelvic pain aren’t
tomies?
cured by a hysterectomy, and so this
A:
Hysterectomy is used to treat:
approach can be a permanent mis-
●
Fibroids. More hysterectomies are
take.
done because of fibroids than any
other problem of the uterus. For
Q: Are there any risks?
many women with fibroids, symp-
A:
A hysterectomy involves some major
toms are minimal and require no
and minor risks. Most women do not
treatment. Also, the fibroids often
shrink after menopause. But fibroids
have problems during or after the oper-
can cause heavy bleeding or pain in
ation. Some risks include:
some women.
●
Heavy blood loss, that requires
blood transfusion
●
Endometriosis. This happens
when the tissue lining the inside of
your uterus grows outside the uterus
on your ovaries, fallopian tubes, or
other pelvic or abdominal organs.
When medication and surgery do
not cure endometriosis, a hysterec
-
tomy often is performed.
●
Bowel injury
●
Bladder injury
●
Anesthesia problems (such as
breathing or heart problems)
●
Need to change to abdominal inci-
sion during surgery
●
Wound pulling open
N ATIONAL W OMEN’ S H EALTH I NFORMATION C ENTER
U.S. Department of Health and Human Services, Office on Women’s Health
womenshealth.gov
1-800-994-9662
TDD: 1-888-220-5446
page 3
F REQUENTLY A SKED Q UESTIONS
Q: Can a hysterectomy lower my
●
Vaginal pessary. This is an object
sexual desire?
inserted into the vagina to hold the
A: Women who have had a hysterectomy,
in which one or both ovaries are
removed, can have lowered sexual
womb in place. It may be used as a
temporary or permanent form of
treatment. Vaginal pessaries come in
desire and decreased pleasure and
orgasm. If you have problems with sex
-
ual desire or functioning, talk to your
doctor.
many shapes and sizes, and they
must be fitted for each woman indi
-
vidually.
Talk to your doctor about nonsurgical
treatments to try first. Doing so is real-
Q: Do options other than hysterec-
ly important if the recommendation for
tomy exist?
a hysterectomy is for a reason other
A:
If you have cancer, hysterectomy might
than cancer.
be the only option. But if you have
uterine fibroids, endometriosis or uter-
Q: What should I do if I am told
ine prolapse, there are other treatments
that I need a hysterectomy?
you can try first.
A:
●
Talk to your doctor about your
●
Drug therapy. Certain medications
may lighten heavy uterine bleeding
or correct uterine bleeding that is
not regular. Certain medications can
options. Ask about other treatments
for your condition.
●
Consider getting a second opinion
from another doctor.
help with endometriosis.
●
Ask about possible complications of
●
Endometrial ablation. If you have
surgery.
heavy or irregular uterine bleeding,
this procedure might ease your
●
Keep in mind that every woman is
symptoms. With a special device, a
different and every situation is dif-
doctor uses electricity, heat, or cold
to destroy the lining of your uterus
and stop uterine bleeding.
ferent. A good treatment choice for
one woman may not be good for
another.
●
Uterine artery embolization. For
treating fibroid, this procedure
Q: If my cervix was removed in my
involves blocking the blood supply
hysterectomy, do I still need to
to the tumors. Without blood, the
have Pap tests?
fibroids shrink over time, which can
A: Ask your doctor if you need to have
reduce pain and heavy bleeding.
periodic Pap tests. Regardless of
●
Myomectomy. If you have fibroid
tumors, this surgical procedure
removes the tumors while leaving
whether you need a Pap test or not, all
women who have had a hysterectomy
must continue to have regular gyneco
-
your uterus intact. There’s a risk
logic exams. ■
that the tumors could come back.
N ATIONAL W OMEN’ S H EALTH I NFORMATION C ENTER
U.S. Department of Health and Human Services, Office on Women’s Health
F REQUENTL Y A SKED Q UESTIONS
womenshealth.gov
1-800-994-9662
TDD: 1-888-220-5446
Quality
Center
For more information…
To learn more about hysterectomy, contact the National Women’s Health Information
Center (NWHIC) at 1-800-994-9662 or the following organizations:
Agency for Healthcare Research and
Phone Number(s): (800) 358-9295 for
requesting publications
Internet Address:
http://www.ahrq.gov/consumer
American College of Obstetricians
and Gynecologists (ACOG) Resource
Phone Number(s): (800) 762-2264 x 192
(for publications requests only)
Internet Address: www.acog.org
American College of Surgeons
Phone Number(s): (312) 202-5000
Internet Address: http://www.facs.org
The FAQ was reviewed by
Dr. Edward Trimble, MD, MPH
Head, Gynecologic Cancer Therapeutics & Quality of Cancer Care Therapeutics,
Clinical Investigations Branch
Cancer Therapy Evaluation Program
National Cancer Institute Division of Cancer Treatment and Diagnosis
May 2006
page 4
N ATIONAL W OMEN’ S H EALTH I NFORMATION C ENTER
U.S. Department of Health and Human Services, Office on Women’s Health