Phone: 305-596-3744
Fax: 305-596-3676
www.floridaamigos.com
The Association of Minimally
Invasive Gynecologic Surgeons
...dedicated to healthy lifestyles and safe, state-of-the-art surgery for
women of all ages.
The Association is dedicated to safe, state-of-the-
art, innovative surgeries and healthy lifestyles for
women of all ages. In a nurturing, environment,
the physicians and staff strive to promote a part-
nership in your healthcare and make every effort
to bridge the sterile science of diseases with your
emotional, physical, and spiritual needs. Every-
one is confronted with difficult healthcare deci-
sions at one time or another. You’ll want your
physician and staff to have the knowledge, experi-
ence, and sensitivity to guide you safely through
the decision-making process.
The Association for Minimally Invasive Gyneco-
logic Surgeons provides comprehensive gyneco-
logic office and surgical healthcare. The physi-
cians are certified in laparoscopy and hys-
teroscopy and are experts in advanced gyneco-
logic surgery. Doctors Pietro and Whitted are na-
tional speakers, trainers, and researchers in ad-
vanced surgical techniques. In addition, Doctors
Pietro and Whitted are Certified Menopause Clini-
cians who educate, train, and research the sci-
ence of menopause. Finally, they are certified in
advanced colposcopy
Doctors Whitted and Pietro offer expert care in the
following areas:
If you need surgery, the Doctors perform most
gynecologic surgeries with minimally invasive
techniques to reduce hospitalization, recovery,
scarring, discomfort and absence from work in
most cases.
.Laugh,
Cough,
Sneeze,
Jump…
...And still stay dry
Urinary incontinence is the loss of bladder
control, or uncontrolled urine leakage.
If you suffer from this problem, you are not alone.
Over 10 million women in the United States experi-
ence incontinence. The embarrassment and invon-
venience of incontinence keep many women from
enjoying a healthy, active lifestyle. As a result, you
may have stopped doing the activities that you
once enjoyed, such as playing with your children or
grandchildren, jogging, playing tennis or golf, or
traveling. It also may have interfered with your
everyday activities such as shopping, lifting or
walking. Incontinence can make you feel less femi-
nine and less intimate with others. But, wait...there
is good news!
Regain Bladder Control.
Regain Your Life.
Paul A. Pietro MD
R. Wayne Whitted MD, MPH
Marina Santana MMS, PA
Janet Levick, Office Administrator
8740 North Kendall Drive
Suite 101
Miami, Florida 33176-2212
Abnormal Paps (HPV) Fibroids (Leiomyoma)
Abnormal Menstrual Cycles Loss of Urine
Bladder Prolapse Menopause
Chronic Pelvic Pain Ovarian cysts
Endometriosis Rectocele
Ectopic Pregnancy Uterine Prolapse
Family Planning Vaginal Prolapse
***Evaluation and Diagnosis of Gynecologic Cancers
Association of Minimally
Invasive Gynecologic Surgeons
...
dedicated to healthy lifestyles and safe, state-of-the-art, innovative surgery for women of all ages
There are several types of urinary inconti-
nence that affect women.
The most common type is stress incontinence,
which affects one out of every six women over the
age of forty, and commonly causes urine leakage
when coughing, sneezing, laughing, jumping or
running.
Stress incontinence occurs when your vaginal and
pelvic floor muscles stretch and weaken after
childbirth, weight gain, surgery, or any activity that
chronically increases abdominal pressure.. This
stretching causes the neck of the bladder to sag
or drop. In this lowered position, the bladder neck
can’t stay closed when abdominal pressure in-
creases during coughing, sneezing and physical
activity. As a result, urine leaks out.
Stress incontinence is not a normal part of aging.
It is a medical problem that can be treated and
even cured for most women. This is the only in-
continence that surgery can cure.
Urge incontinence is another type. Women who
suffer from urge incontinence have an incredible
urge to void and often leak on their way to the
bathroom. Sometimes they leak without warning.
It is also common to experience a combination of
stress and urge, or mixed incontinence. There are
other, more infrequent types of incontinence, as
well. The loss of bladder control most often,
though, is a result of stress incontinence.
What can I do about Incontinence?
The first thing to do is see a doctor who under-
stands the issues of incontinence.
A physical exam, a complete medical history and thor-
ough testing will tell you what is causing your problem.
Then, your doctor can tell you what treatment, or combi-
nation of treatments, is best for you.
The following are non-surgical choices currently avail-
able to treat stress and urge incontinence:
FEMININE PADS, PESSARIES,
AND CATHETERS
Many women who try pads find that they are embar-
rassing, inconvenient, and expensive. Long-term use
can lead to bladder infections and skin irritation. Pes-
saries are small plastic supports which arer inserted into
the vagina to support the bladder. Catheters are in-
serted into the bladder through the urethra to capture
urine. Pessaries and catheters give only temporary
relief and can be irritating to wear.
MEDICATIONS
Medications typically improve urge incontinence. These
include estrogens, bladder anti-spasmodics (detrol,
ditropan, etc.),
Medications for stress incontinence are being investi-
gated. Duloxetine is approaching FDA approval and will
likely be available in the next year.
AVOIDANCE OF BLADDER IRRITANTS
Foods that are acidic are considered irritants. These
are:
Alcoholic beverages, Apples and Juice, Cantaloupe,
Carbonated Beverages, Chili and spicy foods, Citrus
Fruits, Chocolate, Coffee (even decaffeinated), Cran-
berry Juice, Grapes, Guava, Peaches, Pineapple,
Plums, Strawberries, Sugar, Tea, Tomatoes, Vitamin B
Complex, Vinegar.
Low-acid substitutes include: apricots, papaya, pears,
watermelon. Coffee drinkers can drink Kava or Postem.
Tea drinkers can use non-citrus herbal and sun-brewed
teas.
KEGEL EXERCISES
These strengthen the pelvic floor muscles that support
the bladder. In mild incontinence cases improvement is
seen in 60%. 75 exercises per day should be per-
formed for 3 months before improvement is seen.
BLADDER TRAINING
Retraining the bladder can be difficult. In short, when
you get an urge to void you attempt to suppress the
urge with a kegel exercise and distraction prolonging
the interval each week until voiding occurs 6-8
times/day.
SURGICAL OPTIONS ARE FOR STRESS
INCONTINENCE ONLY!
There are over 200 de-
scribed stress incontinence surgeries. The following
are the most effective and are minimally invasive.
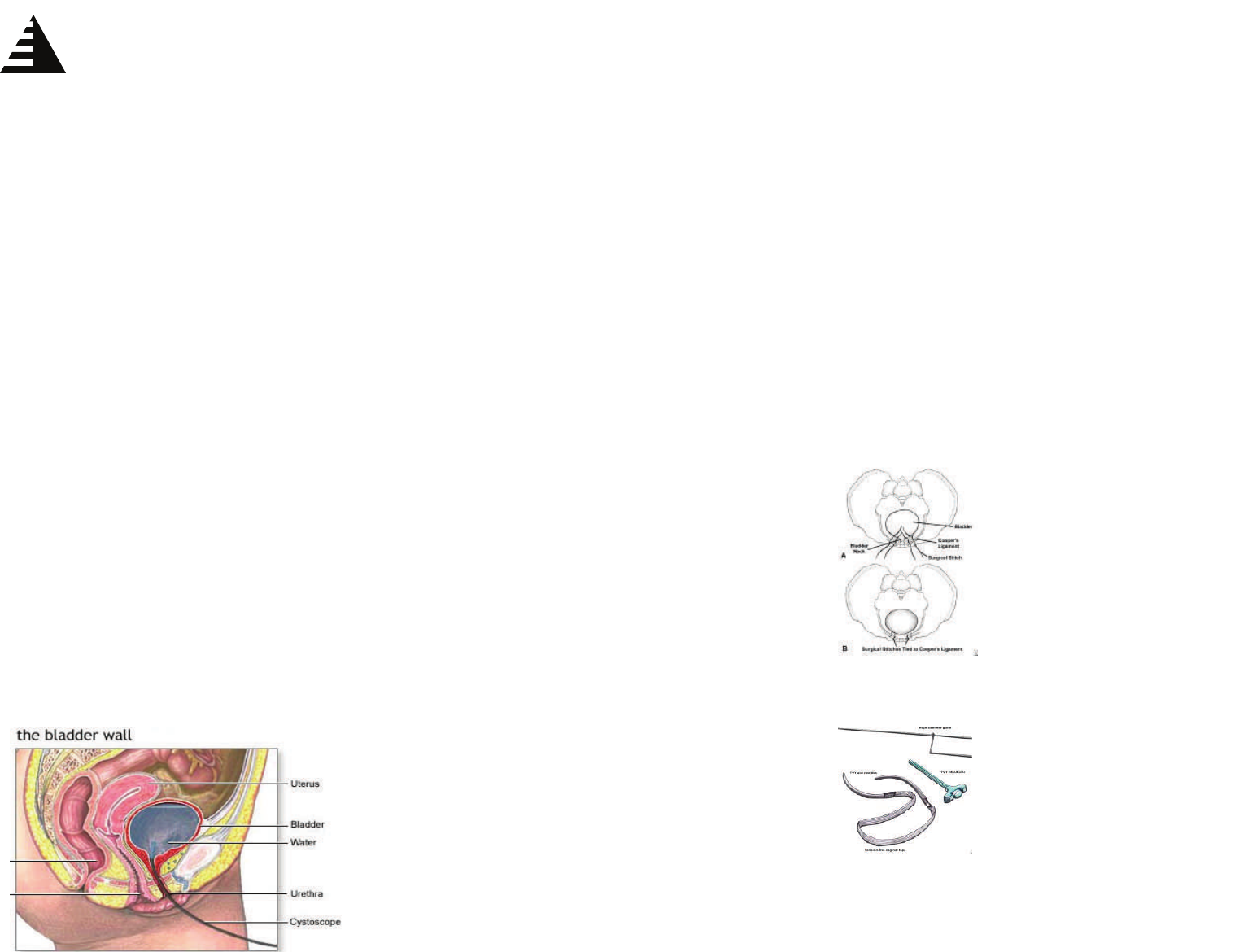
The Laparoscopic Burch Bladder Neck Suspension
The Tension-Free Vaginal Tape Sling Operation
These operations usually are outpatient and require
minimal recovery.
In this procedure the
space between the pubic
bone and the bladder is
dissected. Sutures are
placed in the peri-
bladder-urethral fascia
and attached to the Coo-
per”s ligament on the Pu-
bic Bone. This procedure
has an 80% 5 years suc-
cess rate.
A synthetic mesh is placed
under the mid-portion of the
urethra and and sus-
pended above the pubic
bone. It has a 85-90% cure
rate at 5 years.